Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Liberated Bride by AB Yehoshua - Discussion QuestionsДокумент2 страницыThe Liberated Bride by AB Yehoshua - Discussion QuestionsHoughton Mifflin HarcourtОценок пока нет
- E Content RiyaДокумент8 страницE Content RiyaAnn riya RajanОценок пока нет
- Texas Family Law Update 2013Документ33 страницыTexas Family Law Update 2013Richard R. Orsinger100% (1)
- Families Caring For An Aging AmericaДокумент366 страницFamilies Caring For An Aging AmericaVladimirОценок пока нет
- SPECIAL POWER OF ATTORNEY RhandieДокумент2 страницыSPECIAL POWER OF ATTORNEY RhandieJethmal DayaldasОценок пока нет
- Writing TestДокумент3 страницыWriting TestMax MakarenkoОценок пока нет
- Republic of The PhilippinesДокумент40 страницRepublic of The Philippinesrussell apura galvezОценок пока нет
- Lesson PlanДокумент3 страницыLesson PlanStoica Mirela100% (1)
- Classification of Pteridophytes PDFДокумент15 страницClassification of Pteridophytes PDFsobjanta tech and unboxingОценок пока нет
- Dialogue About A Patient AdmissionДокумент3 страницыDialogue About A Patient AdmissionNila Wardana80% (10)
- LDS Handbook - Book 2 - 08702 - EngДокумент225 страницLDS Handbook - Book 2 - 08702 - EngJohn Waters100% (1)
- Speakout DVD Extra Intermediate Unit 06 PDFДокумент1 страницаSpeakout DVD Extra Intermediate Unit 06 PDFShwe Maw Kun100% (1)
- ESICДокумент24 страницыESICIsha Sushil Bhambi100% (1)
- Indiana Licensed Child Care Center ListingДокумент39 страницIndiana Licensed Child Care Center ListingRandy HoweОценок пока нет
- 755th Carl Edward Landmesser - ObitДокумент1 страница755th Carl Edward Landmesser - ObitNancyОценок пока нет
- Reading Comprehension 8°Документ2 страницыReading Comprehension 8°crycodОценок пока нет
- Updated La Frontera - El Viaje Con PapaДокумент4 страницыUpdated La Frontera - El Viaje Con Papaapi-478437938100% (1)
- Bir Form 2305Документ4 страницыBir Form 2305fatmaaleahОценок пока нет
- Teen Pregnancy Prevention Survey: Asian White/Caucasian Black/African American Other Race (Please Name) Latino/HispanicДокумент2 страницыTeen Pregnancy Prevention Survey: Asian White/Caucasian Black/African American Other Race (Please Name) Latino/HispanicenzoОценок пока нет
- Wedding DanceДокумент1 страницаWedding DanceShem RuinaОценок пока нет
- Female As Karta of The FamilyДокумент28 страницFemale As Karta of The Familyjayneelparikh100% (3)
- Lopez-Rodriguez 1990-Patriarchy & Women's Subordination in The PhilippinesДокумент8 страницLopez-Rodriguez 1990-Patriarchy & Women's Subordination in The PhilippinesAngela ResicoОценок пока нет
- (Tài Liệu KYS) U1 TheoryДокумент22 страницы(Tài Liệu KYS) U1 TheoryHùng TrươngОценок пока нет
- Highlights Hello - July 2016Документ16 страницHighlights Hello - July 2016MilenaОценок пока нет
- Social Case Study ReportДокумент3 страницыSocial Case Study ReportHanabusa Kawaii IdouОценок пока нет
- José Marcelo Ejército SRДокумент2 страницыJosé Marcelo Ejército SRRommel P. AbasОценок пока нет
- SINIGANGДокумент11 страницSINIGANGIvanOcon100% (1)
- Data NikДокумент54 страницыData NikBIMA VIDIOОценок пока нет
- Unsung Heroines ListДокумент2 страницыUnsung Heroines Listcarmenb11015616Оценок пока нет
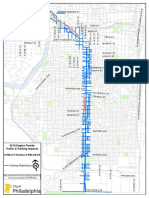
- Eagles Parade Route MapДокумент7 страницEagles Parade Route MapPennLive100% (2)