Вам также может понравиться
- Cause Analysis Manual: Incident Investigation Method & TechniquesОт EverandCause Analysis Manual: Incident Investigation Method & TechniquesОценок пока нет
- Root Cause Analysis Handbook: A Guide to Efficient and Effective Incident InvestigationОт EverandRoot Cause Analysis Handbook: A Guide to Efficient and Effective Incident InvestigationОценок пока нет
- Root Cause AnalysisДокумент9 страницRoot Cause AnalysisAl Engg100% (9)
- Root Cause AnalysisДокумент21 страницаRoot Cause Analysischngan432257% (7)
- Iso22000 2005Документ48 страницIso22000 2005STELLA MARISОценок пока нет
- DOE RCFA Guideline Document PDFДокумент69 страницDOE RCFA Guideline Document PDFrosyidnurdinfauziОценок пока нет
- Asset Integrity Solutions ABBДокумент8 страницAsset Integrity Solutions ABBRInaRIna RinaОценок пока нет
- 4 Ways To Measure Effective Performance of RCAДокумент5 страниц4 Ways To Measure Effective Performance of RCAOsagie AlfredОценок пока нет
- 10 Best Software Tools To Conduct Root Cause Analysis and Solve Complex ProblemsДокумент4 страницы10 Best Software Tools To Conduct Root Cause Analysis and Solve Complex ProblemssaospieОценок пока нет
- IC Explosion at Acme Chemical Company Root Cause Analysis Template Example 0Документ9 страницIC Explosion at Acme Chemical Company Root Cause Analysis Template Example 0Lakhsmie Herawati YuwantinaОценок пока нет
- Root Cause Analysis - ToolДокумент11 страницRoot Cause Analysis - ToolFouzan SoniwalaОценок пока нет
- AI Root Cause AnalysisДокумент27 страницAI Root Cause AnalysisAsuman100% (1)
- Safety Manual: Risk Ranking MatrixДокумент3 страницыSafety Manual: Risk Ranking MatrixMohammed Zubair100% (1)
- Root Cause AnalysisДокумент18 страницRoot Cause AnalysisJohn Brix Balisteros100% (3)
- Análisis Causa Raíz (ACR)Документ281 страницаAnálisis Causa Raíz (ACR)otho107100% (4)
- Eliminating Defects Through Equipment ReliabilityДокумент6 страницEliminating Defects Through Equipment ReliabilityAriefОценок пока нет
- Fmea and FmecaДокумент14 страницFmea and FmecaLindsay SleijpenОценок пока нет
- Equipment Criticality Determination GuidelineДокумент13 страницEquipment Criticality Determination GuidelineMohammed Zubair100% (2)
- Condition Monitoring and Condition Based Maintenance (CBM)Документ9 страницCondition Monitoring and Condition Based Maintenance (CBM)jaggy elgarОценок пока нет
- Engineers View of Human Error - KletzДокумент53 страницыEngineers View of Human Error - KletzRdW992049RdWОценок пока нет
- Risk Based Maintanance PDFДокумент9 страницRisk Based Maintanance PDFRafaelPachecoОценок пока нет
- Skills and Performance StrategyДокумент48 страницSkills and Performance Strategyapi-37986400% (1)
- ZR Handbook For External TI11M00A20-01EДокумент116 страницZR Handbook For External TI11M00A20-01EmiltonОценок пока нет
- Key Elements For Effective RCA & Problem SolvingДокумент76 страницKey Elements For Effective RCA & Problem Solvingdiegocely700615Оценок пока нет
- 5 Critical Factors RCFAДокумент22 страницы5 Critical Factors RCFAKasinathan MuniandiОценок пока нет
- TOR 2014 02202 Root Cause Investigation Best Practices GuideДокумент110 страницTOR 2014 02202 Root Cause Investigation Best Practices GuideOCangaceiro100% (1)
- 2002 Pres 004 BhpbillitonДокумент6 страниц2002 Pres 004 BhpbillitonVan SotОценок пока нет
- Hazard HuntДокумент1 страницаHazard HuntGrace PassiniОценок пока нет
- Corrective-Action Root-Cause Course OutlineДокумент1 страницаCorrective-Action Root-Cause Course OutlineabimanyubawonoОценок пока нет
- Hazard AnalysisДокумент12 страницHazard AnalysisUr FriendОценок пока нет
- Root Cause Analysis MPM1-GlДокумент39 страницRoot Cause Analysis MPM1-GlJunaid KhanОценок пока нет
- Cause and Effect Diagram: CA/PA-RCA: Basic ToolДокумент21 страницаCause and Effect Diagram: CA/PA-RCA: Basic Toolsiddiquiee74100% (1)
- Root Causes AnalisysДокумент33 страницыRoot Causes Analisysandrés_donossoОценок пока нет
- COMET Participant Manual Content Rev - 1Документ116 страницCOMET Participant Manual Content Rev - 1Ángel Alberto Mathieu HanoОценок пока нет
- Fish Bone AnalysisДокумент21 страницаFish Bone AnalysisDeeksha RainaОценок пока нет
- Root Cause AnalysisДокумент105 страницRoot Cause AnalysisJay R Ballon100% (3)
- Bow Tie SafetyДокумент15 страницBow Tie SafetyAshish MishraОценок пока нет
- Root Cause Analysis by MonicaДокумент19 страницRoot Cause Analysis by MonicaMonica B100% (1)
- Session 5-Fault Tree AnalysisДокумент48 страницSession 5-Fault Tree Analysisawang_nasuhaОценок пока нет
- Inherently Safer Design Into PHAДокумент5 страницInherently Safer Design Into PHAManikandan BalasubramanianОценок пока нет
- Root Cause Analysis - Tools and Process: Charles Cotter 15-16 MAY 2014Документ40 страницRoot Cause Analysis - Tools and Process: Charles Cotter 15-16 MAY 2014Eleanore ChavezОценок пока нет
- ISO 14000 Environmental Management SystemsДокумент28 страницISO 14000 Environmental Management Systemssmacky777100% (1)
- Fault Tree HandbookДокумент218 страницFault Tree HandbookRenzo Delgado100% (1)
- MOC Requirement Guidelines and ExamplesДокумент5 страницMOC Requirement Guidelines and ExamplesMohammed ZubairОценок пока нет
- RSSB Investigation Guidance Part 3Документ40 страницRSSB Investigation Guidance Part 3Abdulhmeed MutalatОценок пока нет
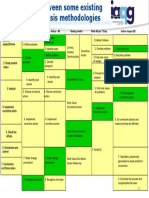
- Root Cause Analysis Methodologies IAQGДокумент1 страницаRoot Cause Analysis Methodologies IAQGAldo100% (1)
- Hopkins Thinking About Process Safety IndicatorsДокумент16 страницHopkins Thinking About Process Safety Indicatorsbinapaniki6520100% (1)
- Root Cause Analysis PresentationДокумент37 страницRoot Cause Analysis PresentationucheonixОценок пока нет
- 7 Secrets of TapRoot RCAДокумент2 страницы7 Secrets of TapRoot RCAMCC2604100% (1)
- SafetyCaseGuidelines PDFДокумент190 страницSafetyCaseGuidelines PDFgad480Оценок пока нет
- Rca CheckДокумент34 страницыRca CheckBhella Guntoro100% (1)
- 6 Common Root Cause Analysis MistakesДокумент4 страницы6 Common Root Cause Analysis MistakesLanilyn AngОценок пока нет
- Incident Investigation GuidelinesДокумент9 страницIncident Investigation GuidelinesNur Carrillo67% (3)
- Failure Analysis Methods What, Why and HowДокумент26 страницFailure Analysis Methods What, Why and Howjwpaprk1100% (1)
- Osha 3895Документ3 страницыOsha 3895Kaycee Lyn Pablo BautistaОценок пока нет
- Group 10 Accident Investigation UpdatedДокумент6 страницGroup 10 Accident Investigation UpdatedAikovin ClerigoОценок пока нет
- Group 10 - Accident InvestigationДокумент6 страницGroup 10 - Accident InvestigationAikovin ClerigoОценок пока нет
- Chapter 14 Managing TeamsДокумент24 страницыChapter 14 Managing TeamsmevasОценок пока нет
- Aghayedo, Elmi-Homework 6Документ3 страницыAghayedo, Elmi-Homework 6faizaОценок пока нет
- Lesson PlanДокумент22 страницыLesson PlanHarim Qudsi100% (1)
- Sports CultureДокумент9 страницSports CultureNanbanОценок пока нет
- RSM1165HF.2020-0108 LDT Final Course Outline OeschДокумент7 страницRSM1165HF.2020-0108 LDT Final Course Outline OeschPОценок пока нет
- Unit Test 1Документ2 страницыUnit Test 1Margerie FrueldaОценок пока нет
- Jurnal Internasional - Bright - Cai PDFДокумент10 страницJurnal Internasional - Bright - Cai PDFNur FadilahОценок пока нет
- A. Content Standard: The Learner Demonstrates An Understanding of Basic NailДокумент5 страницA. Content Standard: The Learner Demonstrates An Understanding of Basic NailPrincess Judy ComedaОценок пока нет
- Pre Referral Intervention StrategiesДокумент2 страницыPre Referral Intervention StrategiesStephanie Wong100% (1)
- Life Success Self Test - Based On The Wheel of LifeДокумент5 страницLife Success Self Test - Based On The Wheel of LifeJain SumeetОценок пока нет
- Inter-Country Adoption: Adoption in The PhilippinesДокумент22 страницыInter-Country Adoption: Adoption in The PhilippinesHusayn TamanoОценок пока нет
- J Gray Theorists and TheoriesДокумент7 страницJ Gray Theorists and Theoriesapi-528983071Оценок пока нет
- Analytical Study of The Sautrāntika PhilosophyДокумент30 страницAnalytical Study of The Sautrāntika Philosophymyatchitshin4121Оценок пока нет
- Suite360 DemoДокумент17 страницSuite360 Demoapi-354511981Оценок пока нет
- IPS Poster Award Competition For World CongressДокумент7 страницIPS Poster Award Competition For World CongressInternational Pharmaceutical Students' Federation (IPSF)Оценок пока нет
- Contemporary Week 5 DLLДокумент4 страницыContemporary Week 5 DLLMae Jane Aguilar100% (2)
- Sex Addiction BrochureДокумент2 страницыSex Addiction BrochureELvine GunawanОценок пока нет
- Work Engagement and Job Crafting Siddiqi2015 - Q1 INDX 81Документ16 страницWork Engagement and Job Crafting Siddiqi2015 - Q1 INDX 81Nely Noer SofwatiОценок пока нет
- Properties of A Well Written TextДокумент5 страницProperties of A Well Written TextJoy Villaspin25% (4)
- Leadership & Management: IB Business and ManagementДокумент33 страницыLeadership & Management: IB Business and Managementapi-529669983Оценок пока нет
- Case 5 Human DevelopmentДокумент5 страницCase 5 Human Developmentapi-201648540Оценок пока нет
- A Mystical Technique To Connect With Mahavatar BabajiДокумент5 страницA Mystical Technique To Connect With Mahavatar Babajisubhash75% (4)
- LEVEL 10, Lesson 7Документ15 страницLEVEL 10, Lesson 7alejandra zapataОценок пока нет
- Constructive FeedbackingДокумент11 страницConstructive FeedbackingGOODWIN GALVANОценок пока нет
- 77-Article Text-218-1-10-20220630Документ16 страниц77-Article Text-218-1-10-20220630EDIT VLOGОценок пока нет
- The Effect of General Cognitive Ability, Teamwork KSA's and The Big Five Personality Factors On The Performances of Engineering Design TeamsДокумент142 страницыThe Effect of General Cognitive Ability, Teamwork KSA's and The Big Five Personality Factors On The Performances of Engineering Design TeamsnisadzhariОценок пока нет
- Vedic MathsДокумент11 страницVedic MathsKi SinghОценок пока нет
- Data Analysis AssignmentДокумент4 страницыData Analysis AssignmentManav khannaОценок пока нет
- NegOr Q3 CESC Module5 v2Документ14 страницNegOr Q3 CESC Module5 v2Joevarie JunioОценок пока нет
- 2017-02-21 - Wilson - 1992 - Frege The Royal Road From GeometryДокумент33 страницы2017-02-21 - Wilson - 1992 - Frege The Royal Road From GeometryazonispОценок пока нет