Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Nursing Leadership and Management Prelims Lesson 1-5Документ4 страницыNursing Leadership and Management Prelims Lesson 1-5Paul Christian P. Santos, RN100% (14)
- Bag TechniqueДокумент1 страницаBag TechniqueCarol Neng CalupitanОценок пока нет
- MORE THAN 3000 QUESTION BANK OF Dr. MOHAMED YAHIAДокумент775 страницMORE THAN 3000 QUESTION BANK OF Dr. MOHAMED YAHIAسماح صلاح100% (1)
- Liver Cirrhosis Case PresДокумент77 страницLiver Cirrhosis Case Presmarlx580% (5)
- Immediate DentureДокумент9 страницImmediate Dentureapi-371094867% (3)
- Nasogastric Tube FeedingДокумент3 страницыNasogastric Tube FeedingLawrence Cada NofiesОценок пока нет
- Pharma Reviewer From VinnyДокумент16 страницPharma Reviewer From VinnyKris TejereroОценок пока нет
- Emergency DrugsДокумент17 страницEmergency Drugsapi-3853350100% (12)
- NCM 104 Cellular Aberration Lecture 2007Документ104 страницыNCM 104 Cellular Aberration Lecture 2007Kris TejereroОценок пока нет
- The Little Black Book of Ecg Secrets PDFДокумент12 страницThe Little Black Book of Ecg Secrets PDFamaandreiОценок пока нет
- Endotracheal Intubation & ER Board Exam QuestionsДокумент33 страницыEndotracheal Intubation & ER Board Exam QuestionsJo-Anne Karen Serdeña0% (1)
- Community Health Nursing ReviewerДокумент11 страницCommunity Health Nursing Revieweroxidalaj88% (24)
- Voies D'abord MasqueletДокумент385 страницVoies D'abord MasqueletAlexandru MazurОценок пока нет
- Qa QuestionsДокумент27 страницQa Questionsapi-213108684100% (1)
- Angelito L. Ramos Jr. RN Clinical InstructorДокумент68 страницAngelito L. Ramos Jr. RN Clinical Instructorraymondblade18100% (17)
- Histology RespiДокумент4 страницыHistology RespiKris TejereroОценок пока нет
- Anatomy Lab IdentificationДокумент3 страницыAnatomy Lab IdentificationKris TejereroОценок пока нет
- Germany DE: State of Health in The EUДокумент24 страницыGermany DE: State of Health in The EUKris TejereroОценок пока нет
- PCM (8) Test For Significance (Dr. Tante)Документ151 страницаPCM (8) Test For Significance (Dr. Tante)Kris TejereroОценок пока нет
- Anatomy Lab IdentificationДокумент6 страницAnatomy Lab IdentificationKris TejereroОценок пока нет
- ABC AccomodationДокумент55 страницABC AccomodationKris TejereroОценок пока нет
- MechanicsДокумент10 страницMechanicsKris TejereroОценок пока нет
- Physics Formulas for Pressure, Water Pressure, and TrigonometryДокумент2 страницыPhysics Formulas for Pressure, Water Pressure, and TrigonometryKris TejereroОценок пока нет
- School Stage RoofingДокумент12 страницSchool Stage RoofingKris TejereroОценок пока нет
- Ronel NaireДокумент4 страницыRonel NaireKris TejereroОценок пока нет
- MechanicsДокумент10 страницMechanicsKris TejereroОценок пока нет
- MechanicsДокумент10 страницMechanicsKris TejereroОценок пока нет
- Of The Main Characters in The PlagueДокумент2 страницыOf The Main Characters in The PlagueKris TejereroОценок пока нет
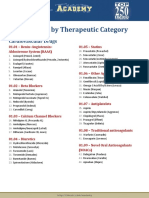
- Drug List by Therapeutic Category: Cardiovascular DrugsДокумент7 страницDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346Оценок пока нет
- Contoh Soal Uji Kompetensi Keperawatan KomunitasДокумент39 страницContoh Soal Uji Kompetensi Keperawatan KomunitasUmairohSetengahTiga67% (3)
- Of The Main Characters in The PlagueДокумент2 страницыOf The Main Characters in The PlagueKris TejereroОценок пока нет
- Cellular AberrationДокумент71 страницаCellular AberrationKris TejereroОценок пока нет
- By: Kris Lyn L. TejereoДокумент30 страницBy: Kris Lyn L. TejereoKris TejereroОценок пока нет
- Level of CompetencyДокумент7 страницLevel of CompetencyKris TejereroОценок пока нет
- HematologyДокумент10 страницHematologyKris TejereroОценок пока нет
- Backbone Drug StudyДокумент1 страницаBackbone Drug StudyKris TejereroОценок пока нет
- Vaccine Minimum Age at 1st Dose Number of Doses Dose Minimum Interval Between Doses Route Site ReasonДокумент4 страницыVaccine Minimum Age at 1st Dose Number of Doses Dose Minimum Interval Between Doses Route Site ReasonKris TejereroОценок пока нет
- Area Inspection Palpation Auscultation Percussion: Physical AssessmentДокумент6 страницArea Inspection Palpation Auscultation Percussion: Physical AssessmentKris TejereroОценок пока нет
- Gastrostomy FeedingДокумент8 страницGastrostomy FeedingToka HessenОценок пока нет
- Weaning Patients With Obesity From Ventilatory Support: ReviewДокумент9 страницWeaning Patients With Obesity From Ventilatory Support: ReviewGian CarloОценок пока нет
- Types of Eyeless NeedlesДокумент13 страницTypes of Eyeless NeedlesClaudia AnissyaОценок пока нет
- Pulse Oximetry v2Документ15 страницPulse Oximetry v2sars_86Оценок пока нет
- Dynamic Changes in Portal Vein Flow During Decongestion in Patients With Heart Failure and Cardio-Renal Syndrome: A POCUS Case SeriesДокумент8 страницDynamic Changes in Portal Vein Flow During Decongestion in Patients With Heart Failure and Cardio-Renal Syndrome: A POCUS Case SeriesMuhammad SyammОценок пока нет
- Intra-op Monitoring ProceduresДокумент4 страницыIntra-op Monitoring ProceduresEsamОценок пока нет
- Atlas of Nerve Conduction Studies and Electromyography (2 Ed.)Документ21 страницаAtlas of Nerve Conduction Studies and Electromyography (2 Ed.)rodrigocorcino899959Оценок пока нет
- HNELHD CG 12 04 Warfarin Age Adjusted Dosing in AdultsДокумент5 страницHNELHD CG 12 04 Warfarin Age Adjusted Dosing in AdultsAnonymous 4txA8N8etОценок пока нет
- Nursing Care of Clients Before and After CABGДокумент46 страницNursing Care of Clients Before and After CABGshejila c hОценок пока нет
- 4 2 - 181 182 PDFДокумент2 страницы4 2 - 181 182 PDFNam LeОценок пока нет
- Unstable Distal Clavicle Fractures (Neer Type II)Документ21 страницаUnstable Distal Clavicle Fractures (Neer Type II)Orthopaedics & Trauma in YoutubeОценок пока нет
- Term 2 Anaphy RatioДокумент40 страницTerm 2 Anaphy RatioAndrea Mae OdquierОценок пока нет
- Recent Advances in Periodontal Surgical Technology: By-Dr Monisha Kaushik 3 Yr MDSДокумент20 страницRecent Advances in Periodontal Surgical Technology: By-Dr Monisha Kaushik 3 Yr MDSmonishakaus24Оценок пока нет
- BiblioДокумент11 страницBiblioNah LaОценок пока нет
- Euac 125Документ23 страницыEuac 125Nicoletta OrphanouОценок пока нет
- Acute Urinary PDFДокумент5 страницAcute Urinary PDFwawanarifkОценок пока нет
- What Is A Pilonidal Sinus, What Causes Them and What Are The Symptoms of Pilonidal SinusДокумент4 страницыWhat Is A Pilonidal Sinus, What Causes Them and What Are The Symptoms of Pilonidal SinusThavam RatnaОценок пока нет
- Rehabilitation After Hip-Joint ReplacementДокумент18 страницRehabilitation After Hip-Joint ReplacementDenise De la CruzОценок пока нет
- Treatment For Spider Veins On LegsДокумент3 страницыTreatment For Spider Veins On LegsZackОценок пока нет
- Experimental and Clinical Reconstructive Microsurgery 1st Ed. 2003 EditionДокумент559 страницExperimental and Clinical Reconstructive Microsurgery 1st Ed. 2003 EditionLuka DamjanovicОценок пока нет
- Presenter Conflict Disclosure SummaryДокумент39 страницPresenter Conflict Disclosure SummaryRirin ChandrikaОценок пока нет
- HA Procedures Respi Heart and PeripheralДокумент10 страницHA Procedures Respi Heart and Peripheralako at ang exoОценок пока нет