Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- AaddДокумент4 страницыAaddSeftri SaputraОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Naskah PublikasiДокумент14 страницNaskah PublikasiSeftri SaputraОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- AaddДокумент4 страницыAaddSeftri SaputraОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- 219 435 1 PBДокумент10 страниц219 435 1 PBWiindha Tahta Alfina CiigejeeОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Kaji Ulang Status Gizi Anak 0-59 Bulan AtmaritaДокумент16 страницKaji Ulang Status Gizi Anak 0-59 Bulan AtmaritaM ZumrodinОценок пока нет
- AaddДокумент4 страницыAaddSeftri SaputraОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Ukuran Lingkar Pergelangan Tangan Sebagai Indikator Kegemukan Pada Anak Usia Sekolah Dasar Di Kota Bogor Jawa BaratДокумент6 страницUkuran Lingkar Pergelangan Tangan Sebagai Indikator Kegemukan Pada Anak Usia Sekolah Dasar Di Kota Bogor Jawa BaratSeftri SaputraОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- 219 435 1 PBДокумент10 страниц219 435 1 PBWiindha Tahta Alfina CiigejeeОценок пока нет
- 29-38 - Jajan PDFДокумент11 страниц29-38 - Jajan PDFSeftri SaputraОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- 219 435 1 PBДокумент10 страниц219 435 1 PBWiindha Tahta Alfina CiigejeeОценок пока нет
- 29-38 - Jajan PDFДокумент11 страниц29-38 - Jajan PDFSeftri SaputraОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- 1 IjahmДокумент10 страниц1 IjahmSeftri SaputraОценок пока нет
- Building System Design Plate 3-Ground Floor PLanДокумент1 страницаBuilding System Design Plate 3-Ground Floor PLanLester de GuzmanОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- 100 Things To Do in Columbia SCДокумент1 страница100 Things To Do in Columbia SCKirk VigilОценок пока нет
- Lca InductionДокумент40 страницLca InductionnualabradyОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Tashelhit Textbook 2011Документ268 страницTashelhit Textbook 2011Massaoud Bicanimen100% (2)
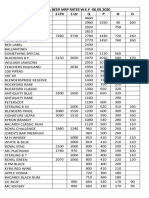
- Liquor & Beer MRP Rates Wef 17.12.2019 (1) - 1Документ2 страницыLiquor & Beer MRP Rates Wef 17.12.2019 (1) - 1Kondu Krishna Vamsi ChowdaryОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Region 5Документ27 страницRegion 5Sheirra SantosОценок пока нет
- Globalization in FisheriesДокумент7 страницGlobalization in Fisheriesnylra MОценок пока нет
- Bryan Babylon Café/Naya International LLCДокумент2 страницыBryan Babylon Café/Naya International LLCKBTXОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Saturday, 07 January 2023Документ4 страницыSaturday, 07 January 2023Ankit padiyarОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hussain Kapadawala 1Документ56 страницHussain Kapadawala 1hussainkapda7276Оценок пока нет
- Company Profile PT - HMSДокумент10 страницCompany Profile PT - HMSmasindraОценок пока нет
- KRON. Food Production - Expanded VersionДокумент47 страницKRON. Food Production - Expanded Versionliuia drusillaОценок пока нет
- Basic Sentence Parts and PatternsДокумент34 страницыBasic Sentence Parts and Patternsapi-327193447100% (1)
- Jurnal DAMPAK PERUBAHAN IKLIM DAN STRATEGI ADAPTASI TANAMAN BUAH DAN SAYURAN DI DAERAH TROPISДокумент12 страницJurnal DAMPAK PERUBAHAN IKLIM DAN STRATEGI ADAPTASI TANAMAN BUAH DAN SAYURAN DI DAERAH TROPISDefani IhsaОценок пока нет
- Menu DietДокумент11 страницMenu DietKrisnaОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Fruit and Vegetable Canning Business PlanДокумент67 страницFruit and Vegetable Canning Business Plankyaq001100% (1)
- Praveenkumar Pol KMF ProjectДокумент57 страницPraveenkumar Pol KMF ProjectPraveenkumar. B. Pol83% (6)
- And The Lion Shall Lie Down With The Lamb: An LDS Member's View of VegetarianismДокумент32 страницыAnd The Lion Shall Lie Down With The Lamb: An LDS Member's View of VegetarianismKevin PomeroyОценок пока нет
- UTS Activity 1Документ12 страницUTS Activity 1Michelle Casayuran - RegalaОценок пока нет
- Fast Moving Consumer GoodsДокумент1 страницаFast Moving Consumer GoodsAshwini ChaudhariОценок пока нет
- Jalgaon IIДокумент9 страницJalgaon IIRam K YadavОценок пока нет
- Leafu PDFДокумент362 страницыLeafu PDFWen RollandОценок пока нет
- Pressure Cooker RecipesДокумент11 страницPressure Cooker RecipesPreeti ChourishiОценок пока нет
- The Awareness of Fast Food Among StudentДокумент8 страницThe Awareness of Fast Food Among StudentCarlsonCarlОценок пока нет
- Northwestern Medicine Modified Consistency Diet April 2016Документ3 страницыNorthwestern Medicine Modified Consistency Diet April 2016sealynОценок пока нет
- Folleto de 3 Caras Informativo para Evento Moderno Gradiente MulticolorДокумент2 страницыFolleto de 3 Caras Informativo para Evento Moderno Gradiente MulticolorBernat Gabarro obiolsОценок пока нет
- Math 10 Module - Q3, WK 4Документ10 страницMath 10 Module - Q3, WK 4Reygie FabrigaОценок пока нет
- The Grandmaster of Demonic CultivationДокумент372 страницыThe Grandmaster of Demonic CultivationSerenity Shizuo100% (2)
- Guidelines For Projects To Be Funded by The TeleFood ProgrammeДокумент5 страницGuidelines For Projects To Be Funded by The TeleFood ProgrammeFaraz Khan RinndОценок пока нет
- BIOL3401 Analysis 6694Документ16 страницBIOL3401 Analysis 6694Rindy SimОценок пока нет