Вам также может понравиться
- Hunger: Mentalization-based Treatments for Eating DisordersОт EverandHunger: Mentalization-based Treatments for Eating DisordersРейтинг: 1 из 5 звезд1/5 (1)
- PB and Eating DisorderДокумент11 страницPB and Eating DisorderKrishnapriya T SОценок пока нет
- Family Functioning and Family Stage Associated With Patterns of Disordered Eating in Adult FemalesДокумент15 страницFamily Functioning and Family Stage Associated With Patterns of Disordered Eating in Adult FemalesAnaОценок пока нет
- CELLA SemДокумент9 страницCELLA Semtatiana CastañedaОценок пока нет
- Parent Gender Affects The Influence of Parent Emotional Eating and Feeding Practices On Child Emotional EatingДокумент12 страницParent Gender Affects The Influence of Parent Emotional Eating and Feeding Practices On Child Emotional EatingStephanie KhouryОценок пока нет
- Basic Family Relations Parental Bonding and DyadicДокумент8 страницBasic Family Relations Parental Bonding and Dyadicsanskriti gautamОценок пока нет
- McCabe, M. & Ricciardelli, L. (2003) .Документ23 страницыMcCabe, M. & Ricciardelli, L. (2003) .P. NoemiОценок пока нет
- Maternal Symptoms of Depression Are Related To Observations of Controlling Feeding Practices in Mothers of Young ChildrenДокумент6 страницMaternal Symptoms of Depression Are Related To Observations of Controlling Feeding Practices in Mothers of Young ChildrenCatarina C.Оценок пока нет
- Maternal Depression Paper 5 3 07 Version For Web PageДокумент45 страницMaternal Depression Paper 5 3 07 Version For Web PageApriyanto Ompu MahmudОценок пока нет
- Impact of Family Pathology On Behavioura PDFДокумент12 страницImpact of Family Pathology On Behavioura PDFAshok KumarОценок пока нет
- Parenting Behaviors Among Anxious and Non Anxious Mothers Relation With Concurrent and Long Term Child OutcomesДокумент20 страницParenting Behaviors Among Anxious and Non Anxious Mothers Relation With Concurrent and Long Term Child OutcomesJust a GirlОценок пока нет
- Junal Asma IIIДокумент14 страницJunal Asma IIIAkfaini MarfirdausОценок пока нет
- Peer and Family Influence in Eating Disorders - A Meta-AnalysisДокумент8 страницPeer and Family Influence in Eating Disorders - A Meta-AnalysisRose MoralesОценок пока нет
- Uq Av 119921Документ15 страницUq Av 119921Epy SaОценок пока нет
- Adolescentes y Depresion MayorДокумент12 страницAdolescentes y Depresion MayorDiana Carolina Vasquez CardenasОценок пока нет
- Chi & Hinshaw 2002 PDFДокумент15 страницChi & Hinshaw 2002 PDFSipkhotunWindayaniОценок пока нет
- 0-3 ReviewДокумент10 страниц0-3 ReviewRolandОценок пока нет
- ART Parenting Styles A Closer Look at A Well-Known ConceptДокумент14 страницART Parenting Styles A Closer Look at A Well-Known ConceptlandrepeОценок пока нет
- Hill 2009Документ12 страницHill 2009Frontier JuniorОценок пока нет
- Nelson 2003Документ16 страницNelson 2003winxukaОценок пока нет
- PT For AdhdДокумент11 страницPT For AdhdAsima MishraОценок пока нет
- Associations Among The Perceived Parent-Child Relationship, Eating Behavior, and Body Weight in Preadolescents: Results From A Community-Based SampleДокумент11 страницAssociations Among The Perceived Parent-Child Relationship, Eating Behavior, and Body Weight in Preadolescents: Results From A Community-Based SamplefpfoОценок пока нет
- Maternal and Paternal Parenting Styles in Adolescents: Associations With Self-Esteem, Depression and Life-SatisfactionДокумент9 страницMaternal and Paternal Parenting Styles in Adolescents: Associations With Self-Esteem, Depression and Life-SatisfactionspaciugОценок пока нет
- Adolescent Grandiose and Vulnerable Narcissism.Документ9 страницAdolescent Grandiose and Vulnerable Narcissism.iqra.nazОценок пока нет
- Art 2021 Metanalálisis Apego y Tea. Sensibilidad MaternaДокумент13 страницArt 2021 Metanalálisis Apego y Tea. Sensibilidad MaternaCarolina GuzmánОценок пока нет
- Examining The Influence of Parenting Practices On Child Psychopathology: A Systematic ReviewДокумент7 страницExamining The Influence of Parenting Practices On Child Psychopathology: A Systematic ReviewPsychology and Education: A Multidisciplinary JournalОценок пока нет
- Family Functioning and Psychological Health of Children With Mentally Ill ParentsДокумент12 страницFamily Functioning and Psychological Health of Children With Mentally Ill ParentsneetiprakashОценок пока нет
- JSW 085Документ12 страницJSW 085Uzman Psikolojik Danışman Aysu BAYRAM SAPTIRОценок пока нет
- Intergeneracionalarticulomiedo PDFДокумент9 страницIntergeneracionalarticulomiedo PDFAcheropita PapazoneОценок пока нет
- Are Attachment Styles DifferentialyДокумент5 страницAre Attachment Styles DifferentialydenisamihaelapsihoОценок пока нет
- Appetite: Charlotte A. Hardman, Paul Christiansen, Laura L. WilkinsonДокумент6 страницAppetite: Charlotte A. Hardman, Paul Christiansen, Laura L. WilkinsonSandu MihaelaОценок пока нет
- Mcgrane 2002 Young Women at Risk For Eating Disorders Perceived Family Dysfunction and Parental Psychological ProblemsДокумент16 страницMcgrane 2002 Young Women at Risk For Eating Disorders Perceived Family Dysfunction and Parental Psychological ProblemsXiloОценок пока нет
- A Longitudinal Study of Parenting Style and Child Weight With Moderation by American Indian EthnicityДокумент27 страницA Longitudinal Study of Parenting Style and Child Weight With Moderation by American Indian EthnicityJelisaaОценок пока нет
- Parenting Stress TheoryДокумент9 страницParenting Stress TheoryPija RamliОценок пока нет
- Positive Parenting Improves Multiple AspectsДокумент11 страницPositive Parenting Improves Multiple Aspectsjuliana_farias_7Оценок пока нет
- Parenting Styles Child BMI and Ratings of Obesigenic Environmen PDFДокумент65 страницParenting Styles Child BMI and Ratings of Obesigenic Environmen PDFHorvath AlexandraОценок пока нет
- Hooper 2011Документ14 страницHooper 2011AdventuRachelОценок пока нет
- 2004 Psychosocial Determinants of Behaviour ProblemsДокумент10 страниц2004 Psychosocial Determinants of Behaviour ProblemsMariajosé CaroОценок пока нет
- Do Friends Share Similar Body Image and Eating Problems TheДокумент21 страницаDo Friends Share Similar Body Image and Eating Problems TheMihaela IonescuОценок пока нет
- 1132 0559 Inter 33 1 0015Документ13 страниц1132 0559 Inter 33 1 0015Abigail MJОценок пока нет
- Resilience in Children of AlcoholicsДокумент6 страницResilience in Children of Alcoholicsdoc_parkerОценок пока нет
- Time Spent With Parents Predicts Change in Depressive Symptoms in Adolescents With Major Depressive DisorderДокумент8 страницTime Spent With Parents Predicts Change in Depressive Symptoms in Adolescents With Major Depressive DisorderHuong Nguyen MaiОценок пока нет
- Invalidating Childhood Environment ScaleДокумент11 страницInvalidating Childhood Environment Scaleanca.tomoroga6627Оценок пока нет
- Chronis 2003Документ9 страницChronis 2003388IHSAN NURОценок пока нет
- Influence of Parent's Eating Attitudes OnДокумент7 страницInfluence of Parent's Eating Attitudes Onfliptik xutxОценок пока нет
- Emotional Co-Regulation Mothers and ChildrenДокумент12 страницEmotional Co-Regulation Mothers and ChildrenAidee NavaОценок пока нет
- Jurnal Stunting 3 B.ingДокумент19 страницJurnal Stunting 3 B.ingAmel afriОценок пока нет
- Protecting Children From The Consequences of Divorce: A Longitudinal Study of The Effects of Parenting On Children's Coping ProcessesДокумент15 страницProtecting Children From The Consequences of Divorce: A Longitudinal Study of The Effects of Parenting On Children's Coping ProcessesAndreea BălanОценок пока нет
- Examining Similarities in Eating Pathology, Negative Affect, and Perfectionism Among Peers. A Social Network AnalysisДокумент8 страницExamining Similarities in Eating Pathology, Negative Affect, and Perfectionism Among Peers. A Social Network AnalysisIrene Sos VilanovaОценок пока нет
- Parent Child Attachment and Problem Behavior Reporting by Mothers With Pathology in Different Socioeconomic StatusДокумент12 страницParent Child Attachment and Problem Behavior Reporting by Mothers With Pathology in Different Socioeconomic StatusSudiptiОценок пока нет
- Factores Proximais Problemas Mentais MaesДокумент21 страницаFactores Proximais Problemas Mentais Maesminha amoraОценок пока нет
- Research ProposalДокумент24 страницыResearch ProposalSaimapari ShaikhОценок пока нет
- Final Research ProposalДокумент18 страницFinal Research Proposalapi-720370980Оценок пока нет
- HHS Public Access: How Parents Describe Picky Eating and Its Impact On Family Meals: A Qualitative AnalysisДокумент17 страницHHS Public Access: How Parents Describe Picky Eating and Its Impact On Family Meals: A Qualitative Analysisyeremias setyawanОценок пока нет
- The Role of Relationship Attachment Styles in Disordered Eating The Role of Relationship Attachment Styles in Disordered Eating Behaviors BehaviorsДокумент11 страницThe Role of Relationship Attachment Styles in Disordered Eating The Role of Relationship Attachment Styles in Disordered Eating Behaviors BehaviorsAlexandra YoanaОценок пока нет
- O24.22.02. Family Well Being and Disabled Children A Psychosocial Model ofДокумент13 страницO24.22.02. Family Well Being and Disabled Children A Psychosocial Model ofLukas LeОценок пока нет
- Brown & Ogden 2004Документ11 страницBrown & Ogden 2004Nurul JamilahОценок пока нет
- Mothers of Undernourished Jamaican Children Have Poorer Psychosocial FunctioningДокумент9 страницMothers of Undernourished Jamaican Children Have Poorer Psychosocial FunctioningJonique TyrellОценок пока нет
- Understanding and Addressing Girls’ Aggressive Behaviour Problems: A Focus on RelationshipsОт EverandUnderstanding and Addressing Girls’ Aggressive Behaviour Problems: A Focus on RelationshipsОценок пока нет
- XI Stoikiometri EnglishДокумент17 страницXI Stoikiometri EnglishZakiyahОценок пока нет
- XI Grafik Titrasi EnglishДокумент11 страницXI Grafik Titrasi EnglishZakiyahОценок пока нет
- XI Stoikiometri EnglishДокумент17 страницXI Stoikiometri EnglishZakiyahОценок пока нет
- XI Part 4 Asam Basa EnglishДокумент10 страницXI Part 4 Asam Basa EnglishZakiyahОценок пока нет
- XI Part 2 Asam Basa EnglishДокумент13 страницXI Part 2 Asam Basa EnglishZakiyahОценок пока нет
- XI Part 3 Asam Basa EnglishДокумент16 страницXI Part 3 Asam Basa EnglishZakiyahОценок пока нет
- XI Part 1 Asam Basa EnglishДокумент13 страницXI Part 1 Asam Basa EnglishZakiyahОценок пока нет
- Exoterm Dan EndotermДокумент19 страницExoterm Dan EndotermZakiyahОценок пока нет
- UntitledДокумент1 страницаUntitledZakiyahОценок пока нет
- UntitledДокумент1 страницаUntitledZakiyahОценок пока нет
- Digital Innovation in Mental HealthДокумент40 страницDigital Innovation in Mental HealthAnshikaSrivastavaОценок пока нет
- Lesson 14 Theories of PersonalityДокумент41 страницаLesson 14 Theories of PersonalityPaula Manalo-SuliguinОценок пока нет
- CHAPTER 7: Mood Disorders and SuicideДокумент13 страницCHAPTER 7: Mood Disorders and SuicideDana Mikaella CervaОценок пока нет
- Agraviador V AgraviadorДокумент2 страницыAgraviador V AgraviadorKim Guevarra100% (1)
- CH 14 Psych DisordersДокумент9 страницCH 14 Psych Disordersюрий локтионовОценок пока нет
- B6 IQ19 - Edward Siderling 2 - STUDENT FINAL 22.23Документ37 страницB6 IQ19 - Edward Siderling 2 - STUDENT FINAL 22.23Bosco785Оценок пока нет
- The Dangers of Gaming A Rhetorical Analysis RevisedДокумент4 страницыThe Dangers of Gaming A Rhetorical Analysis Revisedapi-581677767Оценок пока нет
- THC AspergerДокумент168 страницTHC AspergerMICHAELОценок пока нет
- Nursing TheoriesДокумент376 страницNursing TheoriessanthiyasandyОценок пока нет
- CatharsisДокумент9 страницCatharsisSnowdrops Genevie TanОценок пока нет
- The Assessment InterviewДокумент47 страницThe Assessment InterviewBal Krishna Tharu100% (1)
- Needs Assessment Plan PaperДокумент8 страницNeeds Assessment Plan PaperNaomiОценок пока нет
- 2019 - An Mhealth Intervention For The Treatment of Patients With An Eating Disorder - A Multicenter Randomized Controlled TrialДокумент13 страниц2019 - An Mhealth Intervention For The Treatment of Patients With An Eating Disorder - A Multicenter Randomized Controlled TrialpabobadillaОценок пока нет
- Bibliophobia InglesДокумент4 страницыBibliophobia InglesJoselyn ParedesОценок пока нет
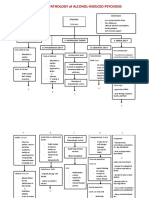
- Psychopathology of Alcohol-Induced Psychosis: EtiologyДокумент3 страницыPsychopathology of Alcohol-Induced Psychosis: EtiologySharlaine CabanayanОценок пока нет
- How To Write A Case HistoryДокумент4 страницыHow To Write A Case HistoryMink's ImranОценок пока нет
- Adhd in Children - Rosile 1Документ10 страницAdhd in Children - Rosile 1api-581754701Оценок пока нет
- Bacp Working With Suicidal Clients Fact Sheet Gpia042Документ18 страницBacp Working With Suicidal Clients Fact Sheet Gpia042Ana MariaОценок пока нет
- VIII - PMHN Role As A Member of The Research TeamДокумент15 страницVIII - PMHN Role As A Member of The Research Teamlester lopezОценок пока нет
- Narcissism: A New TheoryДокумент160 страницNarcissism: A New TheoryGabriela Koestinger100% (15)
- Caso Loretta PDFДокумент24 страницыCaso Loretta PDFIván ToroОценок пока нет
- Selective Mutism, Causes and InterventionsДокумент8 страницSelective Mutism, Causes and InterventionsMartha TriviñoОценок пока нет
- Mental Health First AidДокумент4 страницыMental Health First Aiddskubi8661Оценок пока нет
- Philippine Board of Nursing Course SyllabusДокумент11 страницPhilippine Board of Nursing Course SyllabusChin Chan100% (1)
- Marietta Parker Case No 07-20124-02-JPO Guy and Carrie Neighbors Motion To Revoke Bond Mental Evaluation Cause HearingДокумент58 страницMarietta Parker Case No 07-20124-02-JPO Guy and Carrie Neighbors Motion To Revoke Bond Mental Evaluation Cause HearingJones, WalkerОценок пока нет
- BULIMIAДокумент15 страницBULIMIAMohamedYosefОценок пока нет
- Medical and Psychiatric ComorbiditiesДокумент6 страницMedical and Psychiatric ComorbiditiesDini indrianyОценок пока нет
- Cognitive-Behavioral Theory: A. Antonio González-Prendes and Stella M. ReskoДокумент27 страницCognitive-Behavioral Theory: A. Antonio González-Prendes and Stella M. ReskoRaluca DrbОценок пока нет
- Standard and Innovative Strategies in Cognitive Behavior TherapyДокумент202 страницыStandard and Innovative Strategies in Cognitive Behavior TherapyCaio Rudá de Oliveira100% (4)
- C C CC C C C C C C: Introducing Listening ParticipatingДокумент11 страницC C CC C C C C C C: Introducing Listening ParticipatingRENJULALОценок пока нет