Вам также может понравиться
- Secondary HypertensionОт EverandSecondary HypertensionAlberto MorgantiОценок пока нет
- 12 FullДокумент4 страницы12 FullyesumovsОценок пока нет
- Manejo de La Sepsis 2Документ5 страницManejo de La Sepsis 2Rachmi Pratiwi Febrita PartiОценок пока нет
- Sepsis and The Systemic Inflammatory Response SyndromeДокумент22 страницыSepsis and The Systemic Inflammatory Response SyndromeLaburengkengОценок пока нет
- 11 - Shock - Current Diagnosis and Treatment Emergency MedicineДокумент18 страниц11 - Shock - Current Diagnosis and Treatment Emergency MedicineRon KОценок пока нет
- SepsisДокумент36 страницSepsisWan FaizuddinОценок пока нет
- Dehydration - Background, Pathophysiology, EpidemiologyДокумент4 страницыDehydration - Background, Pathophysiology, EpidemiologyAri GunawanОценок пока нет
- GROUP-6-1Документ48 страницGROUP-6-1baldosangelique14Оценок пока нет
- Circulatory Shock in Children:: An OverviewДокумент10 страницCirculatory Shock in Children:: An Overviewsugarp_3Оценок пока нет
- 13pediatric ConsiderationsДокумент4 страницы13pediatric ConsiderationsIna PoianaОценок пока нет
- Severe Sickle Cell Disease-Pathophysiology and Therapy 2010Документ4 страницыSevere Sickle Cell Disease-Pathophysiology and Therapy 2010Shoua XiongОценок пока нет
- Hemorrhagic Shock PDFДокумент4 страницыHemorrhagic Shock PDFAdreiTheTripleAОценок пока нет
- Refeeding Syndrome A Literature Review KhanДокумент7 страницRefeeding Syndrome A Literature Review Khangw060qpy100% (1)
- Idiopathic Thrombocytopenic Purpura (ITP)Документ7 страницIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiОценок пока нет
- Verma 2009Документ15 страницVerma 2009Zorobabel AzondogaОценок пока нет
- NCBI Bookshelf-Diabetes InsipidusДокумент44 страницыNCBI Bookshelf-Diabetes InsipidusDiah Pradnya ParamitaОценок пока нет
- Managing Pediatric Shock in the Emergency DepartmentДокумент14 страницManaging Pediatric Shock in the Emergency DepartmentAura María Salazar SolarteОценок пока нет
- Pediatric Acute Transverse Myelitis Overview and Differential DiagnosisДокумент12 страницPediatric Acute Transverse Myelitis Overview and Differential Diagnosismmoraes0709Оценок пока нет
- Generalized Convulsive Status Epilepticus in Adults and Children Treatment Guidelines and ProtocolsReviewДокумент14 страницGeneralized Convulsive Status Epilepticus in Adults and Children Treatment Guidelines and ProtocolsReviewAribeth PeñalozaОценок пока нет
- Study of Etiology LALAJUNДокумент3 страницыStudy of Etiology LALAJUNDavid Al HavizОценок пока нет
- Sickle CellДокумент16 страницSickle CellAnastasiafynnОценок пока нет
- Hanhan 2001Документ12 страницHanhan 2001ATIKAH NUR HAFIZHAHОценок пока нет
- Management of Sepsis: Early ResuscitationДокумент16 страницManagement of Sepsis: Early ResuscitationLuis DiazОценок пока нет
- Current Treatment of Pediatric SepsisДокумент3 страницыCurrent Treatment of Pediatric SepsisrulisakaroziОценок пока нет
- Practice ParametersДокумент48 страницPractice Parametersmisbah_mdОценок пока нет
- Critical Synopsis in Brain Death Determination: A Case Report of Brain Death.Документ3 страницыCritical Synopsis in Brain Death Determination: A Case Report of Brain Death.Jhan SaavedraОценок пока нет
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Документ17 страницKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaОценок пока нет
- Lewis: Medical-Surgical Nursing, 10 Edition: Shock, Sepsis, and Multiple Organ Dysfunction Syndrome Key Points ShockДокумент5 страницLewis: Medical-Surgical Nursing, 10 Edition: Shock, Sepsis, and Multiple Organ Dysfunction Syndrome Key Points Shockann forsyОценок пока нет
- Shock, Sepsis, and MODSДокумент5 страницShock, Sepsis, and MODSIndra TimsinaОценок пока нет
- HIE and CVSДокумент11 страницHIE and CVSakshayajainaОценок пока нет
- 1179 Full PDFДокумент10 страниц1179 Full PDFSonia RogersОценок пока нет
- Clinical Manifestation in Sickle Cell Anemia: A Study in Chhattisgarh Institute of Medical Sciences (CIMS) Bilaspur, Chhattisgarh, India.Документ4 страницыClinical Manifestation in Sickle Cell Anemia: A Study in Chhattisgarh Institute of Medical Sciences (CIMS) Bilaspur, Chhattisgarh, India.IOSRjournalОценок пока нет
- Ruiz-Iraztorza Et Al (2010) - Antiphospholipid SyndromeДокумент13 страницRuiz-Iraztorza Et Al (2010) - Antiphospholipid SyndromextraqrkyОценок пока нет
- Fluid and Electrolyte Management For The Surgical PatientДокумент17 страницFluid and Electrolyte Management For The Surgical PatientFery López NavedaОценок пока нет
- Assignment 1 Pathology Aplastic Anemia: Supervisor: DR - Ramez Al-KeelaniДокумент6 страницAssignment 1 Pathology Aplastic Anemia: Supervisor: DR - Ramez Al-Keelaniameer mousaОценок пока нет
- Evidence Based Reading - FormatДокумент2 страницыEvidence Based Reading - FormatMarvie TorralbaОценок пока нет
- Fluid Challenge RevisitedДокумент5 страницFluid Challenge RevisitedNinda DevitaОценок пока нет
- Manejo Choque Septico y Sepsis GraveДокумент17 страницManejo Choque Septico y Sepsis GravewilliamsbarriosОценок пока нет
- Addison Disease: Diagnosis and Initial ManagementДокумент5 страницAddison Disease: Diagnosis and Initial ManagementI Gede SubagiaОценок пока нет
- Evidence Based Reading FormatДокумент2 страницыEvidence Based Reading FormatMarvie TorralbaОценок пока нет
- Case Write Up Emergency Medicine Y5Документ6 страницCase Write Up Emergency Medicine Y5Vaishnevi RajОценок пока нет
- SickleДокумент6 страницSickleNalini T GanesanОценок пока нет
- Status Epilepticus: Current Understanding: D P, M A M C, D GR M C, G, M PДокумент17 страницStatus Epilepticus: Current Understanding: D P, M A M C, D GR M C, G, M PDMishraОценок пока нет
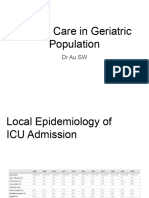
- GeriДокумент61 страницаGeriB AuОценок пока нет
- Cardiovascular and Hematologic Disorders in ChildrenДокумент5 страницCardiovascular and Hematologic Disorders in ChildrenDeekayОценок пока нет
- Septic Shock: by Nsubuga Ivan BMS/12264/182/DU 4.2Документ55 страницSeptic Shock: by Nsubuga Ivan BMS/12264/182/DU 4.2Nsubuga IvanОценок пока нет
- Understanding seizures in diabetesДокумент6 страницUnderstanding seizures in diabetessohailsuОценок пока нет
- Jurnal Kedokteran Dan Kesehatan Indonesia: Association Between Malnutrition and StrokeДокумент7 страницJurnal Kedokteran Dan Kesehatan Indonesia: Association Between Malnutrition and StrokeAditya BatlajeryОценок пока нет
- Editorial: Editorial Current Drug Targets, 2007, Vol. 8, No. 4 491Документ76 страницEditorial: Editorial Current Drug Targets, 2007, Vol. 8, No. 4 491laraalvarenga5832Оценок пока нет
- Summary of Summary 5Документ36 страницSummary of Summary 5anon-265120100% (2)
- Abstract Case PresДокумент6 страницAbstract Case PresSMJ DRDОценок пока нет
- Chapter 67 Shock, SIRS, MODSДокумент5 страницChapter 67 Shock, SIRS, MODSMonica100% (1)
- Evidence-Based Management of Severe Sepsis and Septic ShockДокумент8 страницEvidence-Based Management of Severe Sepsis and Septic ShockFra1312Оценок пока нет
- Distributive ShockДокумент26 страницDistributive ShockYorim Sora PasilaОценок пока нет
- Cardiomiopatia Periparto 2017Документ3 страницыCardiomiopatia Periparto 2017Gustavo Reyes QuezadaОценок пока нет
- Adrenal Senior 1Документ12 страницAdrenal Senior 1mohammad saifuddinОценок пока нет
- Share Explore Search You Slideshare Upload Login Signup Search Submit Search Home Explore Sharelikesave Next SlidesharesДокумент7 страницShare Explore Search You Slideshare Upload Login Signup Search Submit Search Home Explore Sharelikesave Next Slidesharesfaizafazal.900Оценок пока нет
- Therapy PulmonologyДокумент22 страницыTherapy PulmonologyCavinpal SinghОценок пока нет
- Peripheral Retinal Degenerations and Their ManagementДокумент32 страницыPeripheral Retinal Degenerations and Their Managementmanognaaaa100% (1)
- Health Teaching PlanДокумент3 страницыHealth Teaching PlanditamandaОценок пока нет
- Paliative CareДокумент402 страницыPaliative CarewardahОценок пока нет
- Peripheral Vascular DiseaseДокумент53 страницыPeripheral Vascular DiseaseShenbagam Mahalingam100% (1)
- A Case Study On The Ayurvedic Management of Cerebral PalsyДокумент10 страницA Case Study On The Ayurvedic Management of Cerebral PalsyHiramandalam PatanjaliОценок пока нет
- ENT MCQs Eiad NahlaДокумент11 страницENT MCQs Eiad Nahlaadham bani younesОценок пока нет
- Desiccated Origanum Vulgare As Coil Against Aedes AegyptiДокумент27 страницDesiccated Origanum Vulgare As Coil Against Aedes AegyptiEyelessJean12Оценок пока нет
- Lecture Aid: Mental Health and Psychiatric Nursing 1Документ3 страницыLecture Aid: Mental Health and Psychiatric Nursing 1Hershey LerionОценок пока нет
- Avian Influenza (AI) : Synonyms DefinitionДокумент16 страницAvian Influenza (AI) : Synonyms DefinitionDr-Hassan Saeed100% (1)
- The 25 Golden Rules of RunningДокумент10 страницThe 25 Golden Rules of RunningvivektonapiОценок пока нет
- GERD Algorithm Review Definition and Pathophysiology: NO YESДокумент3 страницыGERD Algorithm Review Definition and Pathophysiology: NO YESdianyОценок пока нет
- Medicine2 - Myeloproliferative, Lymphoproliferative WorkshopДокумент118 страницMedicine2 - Myeloproliferative, Lymphoproliferative Workshopapi-3762917100% (1)
- Educating Learners Chapter 9Документ50 страницEducating Learners Chapter 9Allyssa Lorraine PrudencioОценок пока нет
- Copd Copd: What Is COPD? Risk FactorsДокумент1 страницаCopd Copd: What Is COPD? Risk FactorsSirikit MaddelaОценок пока нет
- Human Behavior & Victimology FactorsДокумент25 страницHuman Behavior & Victimology FactorsAyessa Maycie Manuel OlgueraОценок пока нет
- CVJ anatomy classification and clinical signsДокумент53 страницыCVJ anatomy classification and clinical signssa2tigОценок пока нет
- National Institute On Aging Publications CatalogДокумент32 страницыNational Institute On Aging Publications CatalogAbex ComprasОценок пока нет
- Temporomandibular Joint DisordersДокумент46 страницTemporomandibular Joint DisordersTony LeeОценок пока нет
- Oscar Wilde - The Importance of Being EarnestДокумент79 страницOscar Wilde - The Importance of Being EarnestIvo Pires Das Neves100% (2)
- Heart PathologyДокумент8 страницHeart PathologyJose SirittОценок пока нет
- Semiology 998Документ121 страницаSemiology 998Popescu Nicusor100% (1)
- Leprominium A Glimpse With Comparative Study (Nosode of Leprosy)Документ3 страницыLeprominium A Glimpse With Comparative Study (Nosode of Leprosy)Homoeopathic Pulse100% (3)
- The GPHC Question List Jun17-Mch21Документ35 страницThe GPHC Question List Jun17-Mch21Patrick MathewОценок пока нет
- MP SuccessfulPersonalTrainerДокумент14 страницMP SuccessfulPersonalTrainerAnthony Dinicolantonio100% (1)
- Mental Health Effects of ObesityДокумент7 страницMental Health Effects of ObesityMohd FaizОценок пока нет
- Understanding the Mind-Body Link in Chronic IllnessДокумент3 страницыUnderstanding the Mind-Body Link in Chronic IllnessJitendra SinghОценок пока нет
- SchizoДокумент21 страницаSchizoZulkufli YatОценок пока нет
- BlacklegДокумент7 страницBlacklegKoala SpeakОценок пока нет