Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Adrenal Gland - Physiology, Pathology, and Pharmacology - Lecturio PDFДокумент8 страницAdrenal Gland - Physiology, Pathology, and Pharmacology - Lecturio PDFfaiz alamОценок пока нет
- Oet Online - Reading Test 4 A4: 9-If A Hashimoto's Patient Has High Blood Pressure, What Does It Usually Indicate?Документ2 страницыOet Online - Reading Test 4 A4: 9-If A Hashimoto's Patient Has High Blood Pressure, What Does It Usually Indicate?Vistaa SunnyОценок пока нет
- Endocrinology Lab ReportДокумент10 страницEndocrinology Lab Reportapi-285297202Оценок пока нет
- Thyroid GlandДокумент30 страницThyroid GlandahmedkomranОценок пока нет
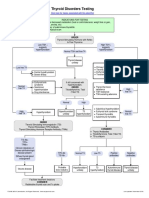
- Thyroid Testing AlgorithmДокумент1 страницаThyroid Testing AlgorithmRezi HelperОценок пока нет
- KKPMT EndokrinДокумент6 страницKKPMT EndokrinDyah CitraОценок пока нет
- Manifestasi Kulit DAN HipotiroidДокумент26 страницManifestasi Kulit DAN HipotiroidAa SsОценок пока нет
- Sciences2lp ModakiratДокумент29 страницSciences2lp Modakiratapi-24974205850% (4)
- HipertiroidДокумент42 страницыHipertiroidCoass XII BonamОценок пока нет
- Diasino Thyroid Test Solutions: Help Raise Thyroid Health AwarenessДокумент2 страницыDiasino Thyroid Test Solutions: Help Raise Thyroid Health AwarenessAbdalazeez AlsayedОценок пока нет
- Performance Task 1Документ3 страницыPerformance Task 1Jellie May RomeroОценок пока нет
- Reproductive Processes: Chapter-34-Lesson-2 Page-961-966Документ26 страницReproductive Processes: Chapter-34-Lesson-2 Page-961-966JanaОценок пока нет
- Anatomy & Physiology of Endocrine SystemДокумент34 страницыAnatomy & Physiology of Endocrine SystemUzma Khan100% (1)
- 015 Physiology MCQ ACEM Primary EndocrineДокумент11 страниц015 Physiology MCQ ACEM Primary Endocrinesandesh100% (1)
- Stages of Lactation ExplainedДокумент35 страницStages of Lactation ExplainedIgnacio FelicityОценок пока нет
- What Is Hormonal ImbalanceДокумент2 страницыWhat Is Hormonal ImbalancestimunoОценок пока нет
- Endocrine System ExplainedДокумент18 страницEndocrine System ExplainedMerlintaОценок пока нет
- Vitamin D and Thyroid Test ResultsДокумент4 страницыVitamin D and Thyroid Test ResultsEkta SinhaОценок пока нет
- MenstrualcyclelecturedrirabonДокумент32 страницыMenstrualcyclelecturedrirabonHananya ManroeОценок пока нет
- Integumentary System TortoraДокумент24 страницыIntegumentary System TortorasyafiqahОценок пока нет
- Pathology of Thyroid DiseasesДокумент5 страницPathology of Thyroid DiseasesGerardLum100% (2)
- TLE Grade-10-3rd-Quarter-Dll-PrДокумент51 страницаTLE Grade-10-3rd-Quarter-Dll-PrMartie AvancenaОценок пока нет
- The skin: the body's largest organДокумент27 страницThe skin: the body's largest organNico Gil GonzalesОценок пока нет
- Endocrine System: Theoretical HandoutДокумент153 страницыEndocrine System: Theoretical HandoutAmy AmyОценок пока нет
- Vphy 143 Lab Experiment 4Документ12 страницVphy 143 Lab Experiment 4Regulus Fidelis SevillaОценок пока нет
- Science 10 - Quiz 1 - Q3W1Документ1 страницаScience 10 - Quiz 1 - Q3W1ChelleОценок пока нет
- Natural World Series Science and Technology Biology.: Heart-The Heart Is A Part of The Circulatory SystemДокумент8 страницNatural World Series Science and Technology Biology.: Heart-The Heart Is A Part of The Circulatory SystemjowieОценок пока нет
- Investigation Observed Value Unit Biological Reference Interval AMH Mullerian Inhibiting Substance 0.185Документ1 страницаInvestigation Observed Value Unit Biological Reference Interval AMH Mullerian Inhibiting Substance 0.185Gangotri GayatriОценок пока нет
- Third Quarter Exam in Science 10Документ3 страницыThird Quarter Exam in Science 10Marife GuadalupeОценок пока нет
- Thyroid Case StudyДокумент68 страницThyroid Case Studyshadydogv5Оценок пока нет