Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The History of Volleyball ProjectДокумент7 страницThe History of Volleyball ProjectEpejema Tagarao Amaro0% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Soccer Formation Lineup Sheet 9v9 332Документ1 страницаSoccer Formation Lineup Sheet 9v9 332Nasrul Azram RamleeОценок пока нет
- Present Simple and Present Continuous: 1. True or FalseДокумент2 страницыPresent Simple and Present Continuous: 1. True or FalseLoredana MagdalenaОценок пока нет
- Ch05 Active Sports and Recreation PDFДокумент12 страницCh05 Active Sports and Recreation PDFRakkard R. NihupaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Bahan Ajar AnnouncementДокумент6 страницBahan Ajar AnnouncementMimi Rahmanita Kuchiki80% (5)
- Reasoning Book PDFДокумент257 страницReasoning Book PDFGauravSingh100% (4)
- Reflection 3 - Physical EducationДокумент4 страницыReflection 3 - Physical Educationapi-321035232Оценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Volleyball EthnographyДокумент6 страницVolleyball EthnographyZachery FollrodОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
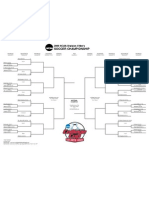
- 2009 Men's Soccer NCAA D1 BracketДокумент1 страница2009 Men's Soccer NCAA D1 Bracket3four3Оценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Badminton Notes PDFДокумент11 страницBadminton Notes PDFAnonymous 5OdZI7R67% (3)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- ResumeДокумент4 страницыResumeapi-490263272Оценок пока нет
- A Person I Really Admire GJ IIIaДокумент4 страницыA Person I Really Admire GJ IIIaJosé Javier BaileОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- FIVB-DeV - 2015 Challenge System GuidelinesДокумент3 страницыFIVB-DeV - 2015 Challenge System GuidelinesLargaespada M NormanОценок пока нет
- Kingston Parks and Recreation Brochure and ReportДокумент55 страницKingston Parks and Recreation Brochure and ReportDaily FreemanОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- William Morgan Invented Volleyball in 1895 at The HolyokeДокумент1 страницаWilliam Morgan Invented Volleyball in 1895 at The HolyokebrettnunezОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- 2007 Annual Report Complete enДокумент212 страниц2007 Annual Report Complete enAkbar KhanОценок пока нет
- The COA-Chronicle May2018 PDFДокумент24 страницыThe COA-Chronicle May2018 PDFnikki.mad8149Оценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Floors For Indoor SportsДокумент20 страницFloors For Indoor SportsrahnemaaОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- 9 Tips To Improve Your DribblingДокумент8 страниц9 Tips To Improve Your DribblingKurt Lubim Alaiza-Anggoto Meltrelez-LibertadОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Handbook For Competitive VolleyballДокумент361 страницаHandbook For Competitive Volleyballarchitectintx100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- SPALDINGДокумент18 страницSPALDINGPuneetОценок пока нет
- Project File: B. L. C. P. Sen. Sec. SchoolДокумент7 страницProject File: B. L. C. P. Sen. Sec. SchoolShivam Kohli100% (1)
- Volleyball Handouts Pe 21Документ5 страницVolleyball Handouts Pe 21Mernafelyn GallemitОценок пока нет
- SMALL SIZED GAMES FOR Soccerintelligence H WEIN PDFДокумент55 страницSMALL SIZED GAMES FOR Soccerintelligence H WEIN PDFbilardox50% (2)
- Strength and Conditioning Coach or Sports Performance Coach or FДокумент3 страницыStrength and Conditioning Coach or Sports Performance Coach or Fapi-121340325Оценок пока нет
- Math Sport 2013 ProceedingsДокумент394 страницыMath Sport 2013 ProceedingsJust Do It.Оценок пока нет
- Ulangan Harian Bahasa Inggris BДокумент3 страницыUlangan Harian Bahasa Inggris BAgita HaryОценок пока нет
- Session 3: Grammar and Writing: Let's PracticeДокумент7 страницSession 3: Grammar and Writing: Let's PracticeevanОценок пока нет
- Second Edition: English For Spanish SpeakersДокумент2 страницыSecond Edition: English For Spanish SpeakersYanareth Federica Cerda CamposОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Lesson Plan 3 Volleyball TroyДокумент6 страницLesson Plan 3 Volleyball Troyapi-487415036100% (1)