Вам также может понравиться
- St. Joseph Mercy Ann Arbor Sepsis Screening ToolДокумент2 страницыSt. Joseph Mercy Ann Arbor Sepsis Screening ToolArnelli HutagalungОценок пока нет
- NHS Lanarkshire Major Haemorrhage GuideДокумент3 страницыNHS Lanarkshire Major Haemorrhage GuideleicesterbugОценок пока нет
- Key points on fluid and electrolyte management, preoperative preparations, and common postoperative complicationsДокумент176 страницKey points on fluid and electrolyte management, preoperative preparations, and common postoperative complicationsAdams AdamОценок пока нет
- مجاهد PDFДокумент176 страницمجاهد PDFHalema Al OkshОценок пока нет
- Mojahid Sheet Complete PDFДокумент176 страницMojahid Sheet Complete PDFOsman SomiОценок пока нет
- Homologous Blood Trasfusion Practice ShortsДокумент23 страницыHomologous Blood Trasfusion Practice ShortsdrprasadingleyОценок пока нет
- Febrile NeutropeniaДокумент1 страницаFebrile Neutropeniaalikarimiak1347Оценок пока нет
- Emily Antes - 2018 Fall MeetДокумент41 страницаEmily Antes - 2018 Fall MeetSyed Shahrul Naz Syed100% (1)
- Blood and Blood Products: Presenter: TAN LI LIAN Supervisor: DR AMINДокумент15 страницBlood and Blood Products: Presenter: TAN LI LIAN Supervisor: DR AMINNur Amin MuhammadОценок пока нет
- Laboratory Blood Request FormДокумент2 страницыLaboratory Blood Request FormIsaac AgbemafleОценок пока нет
- Assessment and Concept Map Care Plan For Critical Care PatientДокумент11 страницAssessment and Concept Map Care Plan For Critical Care Patientapi-604551723Оценок пока нет
- EHC ED Critical Care Induced Hypothermia ProtocolДокумент4 страницыEHC ED Critical Care Induced Hypothermia ProtocolmaddythedocОценок пока нет
- CLINICAL ASPECTS OF BLOOD TRANSFUSIONДокумент37 страницCLINICAL ASPECTS OF BLOOD TRANSFUSIONRaras P P100% (1)
- Admission Criteria Dengue FeverДокумент23 страницыAdmission Criteria Dengue FeverMuhammad Luthfi TaufikОценок пока нет
- Management Guidelines PancreatitisДокумент18 страницManagement Guidelines Pancreatitisfahadrock2002Оценок пока нет
- CRRT Modalities ExplainedДокумент21 страницаCRRT Modalities ExplainedBejo UtomoОценок пока нет
- Case PresentationДокумент22 страницыCase PresentationManjunath ArunachalamОценок пока нет
- Acute Renal Failure CaseДокумент4 страницыAcute Renal Failure CaseMayer RosenbergОценок пока нет
- Chronic Renal FailureДокумент26 страницChronic Renal FailurePriya GandhiОценок пока нет
- Blood Components and Blood TransfusionДокумент38 страницBlood Components and Blood TransfusionjosephОценок пока нет
- Medical Scenario 1Документ42 страницыMedical Scenario 1murphy 1087Оценок пока нет
- Hydatidiform Mole: PGI Sia, Kevin PGI Tan, SheilaДокумент80 страницHydatidiform Mole: PGI Sia, Kevin PGI Tan, SheilaSheila Mary TanОценок пока нет
- Morning Report RIA-1Документ18 страницMorning Report RIA-1RizalMarubobSilalahiОценок пока нет
- CardioДокумент19 страницCardioalsid saningОценок пока нет
- CORONARY ARTERY BYPASS GRAFT Nurse CareДокумент32 страницыCORONARY ARTERY BYPASS GRAFT Nurse CareCharisma Bailey Doody100% (1)
- Dengue TreatmentДокумент10 страницDengue Treatment57 NakshatraОценок пока нет
- High Yield Surgery Compatible VersionДокумент77 страницHigh Yield Surgery Compatible VersionManish K100% (1)
- Noetic ScienceДокумент3 страницыNoetic ScienceMiguel DomingoОценок пока нет
- Case Presentation: EclampsiaДокумент44 страницыCase Presentation: Eclampsiamutiara sitepuОценок пока нет
- Clinical Guideline For Management of Acute Cholecystitis in AdultsДокумент9 страницClinical Guideline For Management of Acute Cholecystitis in AdultsGaby D'LuneОценок пока нет
- Clinical Guideline For Management of Acute Cholecystitis in AdultsДокумент9 страницClinical Guideline For Management of Acute Cholecystitis in AdultsPutria Rezki ArgathyaОценок пока нет
- Managing Diabetic KetoacidosisДокумент9 страницManaging Diabetic KetoacidosisMohammedОценок пока нет
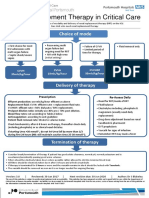
- Renal Replacement Therapy in Critical Care: Choice of ModeДокумент15 страницRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaОценок пока нет
- Anesthesia Post OP OrdersДокумент6 страницAnesthesia Post OP OrdersFaye TinimbangОценок пока нет
- Clinical Guideline For Management of Acute Pancreatitis in AdultsДокумент13 страницClinical Guideline For Management of Acute Pancreatitis in AdultsrivaldiОценок пока нет
- Case Kehamilan Ektopik TergangguДокумент17 страницCase Kehamilan Ektopik TergangguwilliamОценок пока нет
- Gastrointestinal HaemorrhageДокумент58 страницGastrointestinal HaemorrhageAhmed ElwassiefОценок пока нет
- Surgical Intern Survival GuideДокумент85 страницSurgical Intern Survival Guidesgod34100% (1)
- បទបង្ហាញCPDខេត្តកណ្តាលДокумент160 страницបទបង្ហាញCPDខេត្តកណ្តាលSothea SotakОценок пока нет
- Upper GI BleedДокумент50 страницUpper GI BleedNiladri BanerjeeОценок пока нет
- Bloody vomiting and melena case summariesДокумент16 страницBloody vomiting and melena case summariesmiaОценок пока нет
- Abdominal Trauma ExtДокумент73 страницыAbdominal Trauma ExtKitti KkuОценок пока нет
- High Yield Surgery Compatible VersionДокумент77 страницHigh Yield Surgery Compatible VersionEdgar Soto100% (1)
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungДокумент47 страницKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiОценок пока нет
- Mortality by YvonneДокумент25 страницMortality by YvonneYvonne SiiloОценок пока нет
- A House Officer's Approach To DengueДокумент9 страницA House Officer's Approach To DengueBaihaqi SaharunОценок пока нет
- Lapjag 3 Juli 2017 HansДокумент41 страницаLapjag 3 Juli 2017 HansHans WinardiОценок пока нет
- Adult Diabetic Emergencies Care ProtocolДокумент4 страницыAdult Diabetic Emergencies Care ProtocolvladhdОценок пока нет
- Disseminated Intravascular CoagulationДокумент37 страницDisseminated Intravascular CoagulationMuhammad Adeeb100% (1)
- Pedia Notes - 112923Документ59 страницPedia Notes - 112923RASHEED ALADDIN N GUIOMALAОценок пока нет
- Haematology House Officer GuideДокумент7 страницHaematology House Officer GuidePuzzlingОценок пока нет
- Haematology House Officer GuideДокумент7 страницHaematology House Officer GuidePuzzlingОценок пока нет
- Managing Severe Capecitabine DiarrhoeaДокумент5 страницManaging Severe Capecitabine DiarrhoeaJUAN SEBASTIA RIVERA VILLAMIZARОценок пока нет
- Therapeutics Gastro BlockДокумент23 страницыTherapeutics Gastro BlockAngelique Mae Mortejo SalarzaОценок пока нет
- Exchange TransfusionДокумент35 страницExchange Transfusionsobinjohnpkl100% (2)
- Blood Transfusion: Presented To: Sir Khurram AshfaqДокумент33 страницыBlood Transfusion: Presented To: Sir Khurram AshfaqIJAZ HUSSAINОценок пока нет
- Disseminated Intravascular CoagulationДокумент37 страницDisseminated Intravascular CoagulationhipoclaudioОценок пока нет
- El Tiempo Es Vida. Haga Lo Correcto, en El Momento Adecuado ...Документ23 страницыEl Tiempo Es Vida. Haga Lo Correcto, en El Momento Adecuado ...Emilio Fernandez CenturiónОценок пока нет
- WHO Dengue Classification and Case Management-FlyerДокумент2 страницыWHO Dengue Classification and Case Management-FlyerKathleen DyОценок пока нет
- EBM 20may10 ProcalcitoninДокумент17 страницEBM 20may10 ProcalcitoningrahamabraОценок пока нет
- Evidence Based MedicineДокумент10 страницEvidence Based MedicinegrahamabraОценок пока нет
- Petersen Ucsd PHS, Eis 5-25-2010 97Документ53 страницыPetersen Ucsd PHS, Eis 5-25-2010 97grahamabra100% (1)
- Fifteen Campus Map 2009Документ1 страницаFifteen Campus Map 2009grahamabraОценок пока нет
- ADPKD Feb 10Документ132 страницыADPKD Feb 10grahamabraОценок пока нет
- Quiet Hours Paging PolicyДокумент1 страницаQuiet Hours Paging PolicygrahamabraОценок пока нет
- ABIM Logy Review 2010Документ111 страницABIM Logy Review 2010grahamabraОценок пока нет
- Review Small Bowel Colon: of The ANDДокумент43 страницыReview Small Bowel Colon: of The ANDgrahamabraОценок пока нет
- 6th Central Pay Commission Salary CalculatorДокумент15 страниц6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 2010 Allergy and Immunology Board ReviewДокумент132 страницы2010 Allergy and Immunology Board Reviewgrahamabra50% (2)
- CME JRK Brochure 2010 (10-22)Документ6 страницCME JRK Brochure 2010 (10-22)grahamabraОценок пока нет
- Internal Medicine Board ReviewДокумент64 страницыInternal Medicine Board Reviewgrahamabra50% (2)
- Maputo Morning Report (Kwan) - 1Документ40 страницMaputo Morning Report (Kwan) - 1grahamabraОценок пока нет
- Medical ManagementДокумент24 страницыMedical ManagementgrahamabraОценок пока нет
- 2018 G12 Biology E PDFДокумент402 страницы2018 G12 Biology E PDFAli Shahzad25% (4)
- Paediatric Nephrology Syllabus FinalДокумент13 страницPaediatric Nephrology Syllabus FinalClever BarbieОценок пока нет
- Methanol and Ethylene Glycol Poisoning - Management - UpToDateДокумент16 страницMethanol and Ethylene Glycol Poisoning - Management - UpToDateSandra Diaz ArangoitiaОценок пока нет
- HBN 07-02 FinalДокумент50 страницHBN 07-02 Finalsurantha jayawardanaОценок пока нет
- Usp 38-1231Документ27 страницUsp 38-1231spiderman00Оценок пока нет
- Guangdong Biolight Meditech Co.,Ltd.: Future Healthcare TechnologyДокумент12 страницGuangdong Biolight Meditech Co.,Ltd.: Future Healthcare TechnologyCampaign MediaОценок пока нет
- Vascular Access in Clinical PracticeДокумент443 страницыVascular Access in Clinical PracticeRamona TutunariuОценок пока нет
- Desalting, Concentration, and Buffer Exchange by Dialysis and UltrafiltrationДокумент15 страницDesalting, Concentration, and Buffer Exchange by Dialysis and UltrafiltrationAlejandraBarrónHernándezОценок пока нет
- Topical Issues in Anesthesia 2016Документ207 страницTopical Issues in Anesthesia 2016Ketzalzin DmgОценок пока нет
- HemodialysisДокумент25 страницHemodialysisØsama ĀlarekeОценок пока нет
- Interface Disinfection ProceduresДокумент32 страницыInterface Disinfection ProceduresMagdi FarhanОценок пока нет
- Proposed BGHMC Dialysis Centre to Address Inadequate Renal FacilitiesДокумент6 страницProposed BGHMC Dialysis Centre to Address Inadequate Renal Facilitiesjade cabreraОценок пока нет
- Medical skills checklist for nursesДокумент5 страницMedical skills checklist for nursesHussain R Al-MidaniОценок пока нет
- Evidence Based Practice: Dorothea Orem's Self Care Deficit TheoryДокумент37 страницEvidence Based Practice: Dorothea Orem's Self Care Deficit TheoryVette Angelikka Dela CruzОценок пока нет
- Dialysis CompilationДокумент13 страницDialysis CompilationNurwani HussinОценок пока нет
- End-Stage Renal Disease Kidney Transplantation TopДокумент8 страницEnd-Stage Renal Disease Kidney Transplantation Topmondae175934Оценок пока нет
- Guía para La Prevención de Infecciones Relacionadas Con El Catéter Intravascular 2Документ90 страницGuía para La Prevención de Infecciones Relacionadas Con El Catéter Intravascular 2Jhonny Marquez100% (1)
- IVPN Digest February 2021Документ21 страницаIVPN Digest February 2021Omnia El HossienyОценок пока нет
- Advances in Chronic Kidney Disease 2007 - C. Ronco, N. Levin (Karger, 2007) WWДокумент149 страницAdvances in Chronic Kidney Disease 2007 - C. Ronco, N. Levin (Karger, 2007) WWAbdallah BouleghraifОценок пока нет
- Blood Purif 2015 40 (1) 84-91Документ8 страницBlood Purif 2015 40 (1) 84-91Fabiana SalernoОценок пока нет
- Standard of Nursing ServicesДокумент43 страницыStandard of Nursing ServicesMichael Hall100% (2)
- Supply & installation of furniture for Arab Open UniversityДокумент32 страницыSupply & installation of furniture for Arab Open Universitysec ondoОценок пока нет
- Requirements DialysisclinicДокумент5 страницRequirements DialysiscliniceimrehОценок пока нет
- AK98 Leaflet 4p A4 LowДокумент3 страницыAK98 Leaflet 4p A4 LowJosé GómezОценок пока нет
- PCU Stepdown Skills ChecklistДокумент7 страницPCU Stepdown Skills Checklistnorthweststaffing100% (1)
- Medical Nutrition Therapy For Hemodialysis PatientsДокумент24 страницыMedical Nutrition Therapy For Hemodialysis Patientsraquelt_65Оценок пока нет
- Kdqol 36Документ8 страницKdqol 36Anonymous 8i7BMgОценок пока нет
- BR - Multifiltrate FreseniusДокумент16 страницBR - Multifiltrate FreseniusLeonardo Jose HernandezОценок пока нет
- Hemodialysis Tunneled Catheter-Related Infections: VAWG Vascular Access SeriesДокумент11 страницHemodialysis Tunneled Catheter-Related Infections: VAWG Vascular Access SeriesLuis octavio carranzaОценок пока нет
- IC: The All-Rounder in Pharmaceutical Analysis: Stephanie Kappes, Alfred Steinbach, and Katinka RuthДокумент7 страницIC: The All-Rounder in Pharmaceutical Analysis: Stephanie Kappes, Alfred Steinbach, and Katinka RuthAstrid Carolina Gutierrez ShimabukuroОценок пока нет
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesОт EverandThe Ultimate Guide To Memory Improvement TechniquesРейтинг: 5 из 5 звезд5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementОт EverandTechniques Exercises And Tricks For Memory ImprovementРейтинг: 4.5 из 5 звезд4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОценок пока нет
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОценок пока нет
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 5 из 5 звезд5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingОт EverandThe Happiness Trap: How to Stop Struggling and Start LivingРейтинг: 4 из 5 звезд4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingОт EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingРейтинг: 5 из 5 звезд5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingОт EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingРейтинг: 3.5 из 5 звезд3.5/5 (32)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsОт EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsОценок пока нет
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossОт EverandThe Tennis Partner: A Doctor's Story of Friendship and LossРейтинг: 4.5 из 5 звезд4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisОт EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisРейтинг: 5 из 5 звезд5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisОт EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisРейтинг: 5 из 5 звезд5/5 (8)