Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Reading Comprehension LatihanДокумент3 страницыReading Comprehension LatihanlolatrhesiaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Leslie V FarlandДокумент10 страницLeslie V FarlandtiaranindyОценок пока нет
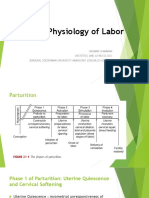
- Physiology of LaborДокумент17 страницPhysiology of Laborsennaavia12Оценок пока нет
- Seminar On Skilled Birth SBA ModuleДокумент50 страницSeminar On Skilled Birth SBA ModuleSangita Patir83% (40)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Breech PDFДокумент4 страницыBreech PDFMiguel Cuevas Dolot100% (1)
- Cesarean Delivery - A Comprehensive Illustrated Practical Guide - 2017 PDFДокумент402 страницыCesarean Delivery - A Comprehensive Illustrated Practical Guide - 2017 PDFDusty Sand100% (1)
- Comprehensive Abortion Care: Dr. Diomede NtasumbumuyangeДокумент42 страницыComprehensive Abortion Care: Dr. Diomede NtasumbumuyangeKate SantosОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- #3 Cesarean SectionДокумент20 страниц#3 Cesarean SectionDunice Lloyd Mata100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Space Proximity - Gynecology and Obstetrics UnitДокумент10 страницSpace Proximity - Gynecology and Obstetrics UnitSheryl ShekinahОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- 985-Article Text-5131-1-10-20220801Документ8 страниц985-Article Text-5131-1-10-20220801armyta ddОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- 18 - Oligohydramnios and PolyhydramniosДокумент3 страницы18 - Oligohydramnios and PolyhydramniosSu OoОценок пока нет
- Kode ICD X Untuk Bagian OBSGINДокумент19 страницKode ICD X Untuk Bagian OBSGINYuyun Caroline100% (1)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- What Are The Reasons For IVF FailureДокумент10 страницWhat Are The Reasons For IVF FailureTone Jarvis-MackОценок пока нет
- IndianJObstetGynecolRes 9-3-335 341Документ7 страницIndianJObstetGynecolRes 9-3-335 341axel jovito siburianОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- AHDP - Teenage Pregnancy NewДокумент20 страницAHDP - Teenage Pregnancy NewEdisa AsuncionОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Molar PregnancyДокумент13 страницMolar PregnancyShalynurОценок пока нет
- Coass in Charge: Fara/Vicia/Yanti/ Eva/Tryas/Desi Supervisor: Dr. Mulyo Hadi Sungkono, SP - OG (K)Документ15 страницCoass in Charge: Fara/Vicia/Yanti/ Eva/Tryas/Desi Supervisor: Dr. Mulyo Hadi Sungkono, SP - OG (K)Tryas YulithaОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Learning Contract 2019 2020 GenapДокумент5 страницLearning Contract 2019 2020 GenapAuliya DiyaaОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Memo On March 25, 1981Документ2 страницыMemo On March 25, 1981grace poudrierОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Ectopic PregnancyДокумент27 страницEctopic PregnancyrowenanuquiОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Unit 7 - Vesicular MoleДокумент43 страницыUnit 7 - Vesicular MoleN. Siva100% (1)
- POLYHYDRAMNIOSДокумент2 страницыPOLYHYDRAMNIOSyxly imperialОценок пока нет
- Seminar On Prolonged PregnancyДокумент3 страницыSeminar On Prolonged PregnancyBHUKYA USHARANIОценок пока нет
- Mapa Ingles RPMДокумент1 страницаMapa Ingles RPMDaniela RodriguezОценок пока нет
- Chapter 2Документ15 страницChapter 2Kkneekkhaii Gallo Jalandra100% (1)
- Part 2 Mrcog Short Answer QuestionsДокумент1 страницаPart 2 Mrcog Short Answer QuestionsDr.Marva YusafzaiОценок пока нет
- Obstetrics Midterms Rationale 2nd Sem 2018 2019Документ21 страницаObstetrics Midterms Rationale 2nd Sem 2018 2019Gene Paulo UyОценок пока нет
- Pregnancy & ChildbirthДокумент12 страницPregnancy & Childbirthrobert tambuliОценок пока нет
- Normal Labour QuizДокумент2 страницыNormal Labour QuizAsh_myОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- PPP NCM 107Документ2 страницыPPP NCM 107Anna YepisОценок пока нет