Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- HP Scanjet N9120 (Service Manual) PDFДокумент394 страницыHP Scanjet N9120 (Service Manual) PDFcamilohto80% (5)
- A First Etymological Dictionary of BasquДокумент29 страницA First Etymological Dictionary of BasquDaily MailОценок пока нет
- SemДокумент583 страницыSemMaria SantosОценок пока нет
- National Pension System (NPS) - Subscriber Registration FormДокумент3 страницыNational Pension System (NPS) - Subscriber Registration FormPratikJagtapОценок пока нет
- Angle ModulationДокумент26 страницAngle ModulationAtish RanjanОценок пока нет
- Optimizing Stata For Analysis of Large Data SetsДокумент29 страницOptimizing Stata For Analysis of Large Data SetsTrần Anh TùngОценок пока нет
- Void Engineers (Convention: Mage The Ascension)Документ6 страницVoid Engineers (Convention: Mage The Ascension)Beth0% (1)
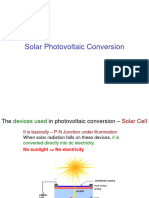
- Slide 7 PV NewДокумент74 страницыSlide 7 PV NewPriyanshu AgrawalОценок пока нет
- 1.2 The Basic Features of Employee's Welfare Measures Are As FollowsДокумент51 страница1.2 The Basic Features of Employee's Welfare Measures Are As FollowsUddipta Bharali100% (1)
- Gates Crimp Data and Dies Manual BandasДокумент138 страницGates Crimp Data and Dies Manual BandasTOQUES00Оценок пока нет
- T54125AДокумент64 страницыT54125ARaúl FroddenОценок пока нет
- Tecsun Pl310et PDFДокумент30 страницTecsun Pl310et PDFAxel BodemannОценок пока нет
- تأثير العناصر الثقافية والبراغماتية الأسلوبية في ترجمة سورة الناس من القرآن الكريم إلى اللغة الإ PDFДокумент36 страницتأثير العناصر الثقافية والبراغماتية الأسلوبية في ترجمة سورة الناس من القرآن الكريم إلى اللغة الإ PDFSofiane DouifiОценок пока нет
- Green ThumbДокумент2 страницыGreen ThumbScarlet Sofia Colmenares VargasОценок пока нет
- Visual Metaphor Process BookДокумент18 страницVisual Metaphor Process Bookmatt8859Оценок пока нет
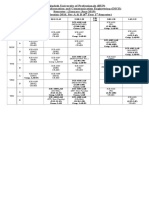
- Class Routine Final 13.12.18Документ7 страницClass Routine Final 13.12.18RakibОценок пока нет
- LQZLQM ) So"L/L6H Klans LN : Sfof (No K - Of) HGSF) Nflu DFQДокумент5 страницLQZLQM ) So"L/L6H Klans LN : Sfof (No K - Of) HGSF) Nflu DFQSAJAL KOIRALAОценок пока нет
- Formulae HandbookДокумент60 страницFormulae Handbookmgvpalma100% (1)
- TOEFL-Reading Question Type Definitions and ExplanationДокумент5 страницTOEFL-Reading Question Type Definitions and ExplanationSamara SampaioОценок пока нет
- Program of ActivitiesДокумент2 страницыProgram of ActivitiesVon Limuel LopezОценок пока нет
- Hexoloy SP Sic TdsДокумент4 страницыHexoloy SP Sic TdsAnonymous r3MoX2ZMTОценок пока нет
- International Supply Chain ManagementДокумент2 страницыInternational Supply Chain ManagementPRASANT KUMAR SAMALОценок пока нет
- Hemax-530 PDFДокумент2 страницыHemax-530 PDFNice BennyОценок пока нет
- Tekla SoakwayДокумент2 страницыTekla SoakwayBalaji Naik100% (1)
- Evidence MODULE 1 Evidence DefinitionДокумент8 страницEvidence MODULE 1 Evidence Definitiondave BarretoОценок пока нет
- InterviewДокумент8 страницInterviewswapnadip kumbharОценок пока нет
- Unit 1 - Plant & Eqpt. Safety Apprisal & Control Techq.Документ147 страницUnit 1 - Plant & Eqpt. Safety Apprisal & Control Techq.Madhan MОценок пока нет
- "Large Quote Goes Here.": Title or Heading HereДокумент2 страницы"Large Quote Goes Here.": Title or Heading HereHesti RianaОценок пока нет
- 74 Series Logic ICsДокумент6 страниц74 Series Logic ICsanon-466841Оценок пока нет
- 2018-2019 Annual Algebra Course 1 Contest: InstructionsДокумент2 страницы2018-2019 Annual Algebra Course 1 Contest: InstructionsNaresh100% (1)