Вам также может понравиться
- Fire Ice and MountainsДокумент23 страницыFire Ice and MountainsRachel DanielsОценок пока нет
- Energy Budget Fall 2017Документ1 страницаEnergy Budget Fall 2017Rachel DanielsОценок пока нет
- Terrestrial: Name Scientific Name History Habitat Impacts Control MethodsДокумент5 страницTerrestrial: Name Scientific Name History Habitat Impacts Control MethodsRachel DanielsОценок пока нет
- Human Physiology WorksheetДокумент4 страницыHuman Physiology WorksheetRachel DanielsОценок пока нет
- Introduction To Chemistry: 1.2 Numbers in ScienceДокумент24 страницыIntroduction To Chemistry: 1.2 Numbers in ScienceRachel DanielsОценок пока нет
- APUSH - Chapter 5 Reading Questions (Unit 2)Документ2 страницыAPUSH - Chapter 5 Reading Questions (Unit 2)Rachel DanielsОценок пока нет
- Reaching Nowhere Else But UpДокумент2 страницыReaching Nowhere Else But UpRachel DanielsОценок пока нет
- By Robert Frost: The Road Not TakenДокумент3 страницыBy Robert Frost: The Road Not TakenRachel DanielsОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Legionella - A Reemerging PathogenДокумент9 страницLegionella - A Reemerging PathogenBam ManОценок пока нет
- Penyuluhan Kesehatan Osteoporosis Pada Lansia Di Posyandu Lansia Anggrek Dusun Nitipuran, Sonosewu, BantulДокумент5 страницPenyuluhan Kesehatan Osteoporosis Pada Lansia Di Posyandu Lansia Anggrek Dusun Nitipuran, Sonosewu, BantulRizky AnalystОценок пока нет
- Role of The Public Health Nurse in The Manila Health DepartmentДокумент2 страницыRole of The Public Health Nurse in The Manila Health DepartmentMaria Joji Sy100% (1)
- Top Questions About Your Menstrual Cycle: When Should I See A Doctor About A Period Problem?Документ2 страницыTop Questions About Your Menstrual Cycle: When Should I See A Doctor About A Period Problem?Kofi YeboahОценок пока нет
- Barangay Health Governance Body 2018Документ44 страницыBarangay Health Governance Body 2018Donna Lei G. RosarioОценок пока нет
- Tle 7-W3Документ1 страницаTle 7-W3Deverly AmplayoОценок пока нет
- Covid 19 QuestionnaireДокумент2 страницыCovid 19 QuestionnaireChristine De Villa-RagudoОценок пока нет
- Knowledge Regarding Cervical Cancer Among Married Women in Rural Telangana: A Cross Sectional StudyДокумент5 страницKnowledge Regarding Cervical Cancer Among Married Women in Rural Telangana: A Cross Sectional StudySrideviRaviОценок пока нет
- Inspirational Birth StoriesДокумент377 страницInspirational Birth Storiescris_c3100% (4)
- Form A - Checklist For Temporary Living Quarters in Factory/Office SpaceДокумент10 страницForm A - Checklist For Temporary Living Quarters in Factory/Office SpaceWanping TangОценок пока нет
- Articulo YangДокумент4 страницыArticulo YangAlekhine Cubas MarinaОценок пока нет
- Safety On Accident Site:: Bloodborne Pathogen AwarenessДокумент69 страницSafety On Accident Site:: Bloodborne Pathogen Awarenessdaily absurdОценок пока нет
- Msoga 1Документ73 страницыMsoga 1gabrielОценок пока нет
- Subgroup 3Документ12 страницSubgroup 3John Mervin OliverosОценок пока нет
- Aids UpdateДокумент40 страницAids UpdateipursОценок пока нет
- Early Incident Reporting TBTДокумент1 страницаEarly Incident Reporting TBTRichard SmithОценок пока нет
- Indikasi SCДокумент11 страницIndikasi SCLutfiAnny Rahman HakimОценок пока нет
- Module 3 Reproductive Life Planning 2023Документ13 страницModule 3 Reproductive Life Planning 2023AinaB ManaloОценок пока нет
- Covid-19 Virus RT-PCR (Open System) Qualitative - Centre VisitДокумент2 страницыCovid-19 Virus RT-PCR (Open System) Qualitative - Centre VisitChinish KalraОценок пока нет
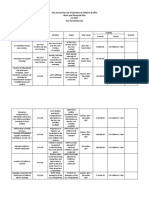
- 2017 CCPC Work and Financial PlanДокумент7 страниц2017 CCPC Work and Financial PlanPatrick Jorge SibayanОценок пока нет
- Baltimore PI MotionДокумент62 страницыBaltimore PI MotionLindsey KaleyОценок пока нет
- DK H 2567 003 FinalPLДокумент5 страницDK H 2567 003 FinalPLArsynОценок пока нет
- OB Practicum Case Study 2Документ4 страницыOB Practicum Case Study 2Trixia DaclesОценок пока нет
- Chicken Pox N C P BY BHERU LALДокумент2 страницыChicken Pox N C P BY BHERU LALBheru Lal100% (1)
- Data Non SpesialistikДокумент20 страницData Non SpesialistikNhiar SaniaОценок пока нет
- Diet and Exercise EffectДокумент5 страницDiet and Exercise Effectsafar akramОценок пока нет
- Skrining Must - WordДокумент3 страницыSkrining Must - WordM Rendy RamadhanОценок пока нет
- Commonucable Diseases EpidemiologyДокумент59 страницCommonucable Diseases Epidemiologyد.شيماءسعيد100% (1)
- Family Planning MethodsДокумент7 страницFamily Planning MethodsAngelika PadawanОценок пока нет
- Pengetahuan, Sikap Dan Etika Batuk Pada Penderita Tuberkulosis ParuДокумент8 страницPengetahuan, Sikap Dan Etika Batuk Pada Penderita Tuberkulosis ParuNurafni LativamcbОценок пока нет