Вам также может понравиться
- Nondestructive TestingДокумент27 страницNondestructive Testingapi-3764139Оценок пока нет
- Sharing Session Piping Material - Flame ArrestorДокумент18 страницSharing Session Piping Material - Flame ArrestorDinda Putri AmaliaОценок пока нет
- Closed Book PortionДокумент5 страницClosed Book Portionvishal bailurОценок пока нет
- Revamp Fired Heaters To Increase Capacity PDFДокумент8 страницRevamp Fired Heaters To Increase Capacity PDFCarrillo RomerОценок пока нет
- 45 Samss 009Документ6 страниц45 Samss 009naruto256Оценок пока нет
- "State-Of-The-Art" Delayed Coking Structure For Frontier RefiningДокумент13 страниц"State-Of-The-Art" Delayed Coking Structure For Frontier Refiningandy175Оценок пока нет
- Engineering Encyclopedia: Exxon Chemical and Mechanical Cleaning Manual 12) Fouling Control by PrepassivationДокумент9 страницEngineering Encyclopedia: Exxon Chemical and Mechanical Cleaning Manual 12) Fouling Control by Prepassivationcvg ertdОценок пока нет
- Flu or Delayed Coking ExperienceДокумент5 страницFlu or Delayed Coking ExperienceLeon SanchezОценок пока нет
- Mogas Data Sheet Purge System Designs (En)Документ7 страницMogas Data Sheet Purge System Designs (En)kumar.arunk6784100% (1)
- CBI Welding Journal Vert Plate Apr04Документ0 страницCBI Welding Journal Vert Plate Apr04Mahendra RathoreОценок пока нет
- Mechanical Completion Procedure for HPCL Visakh ProjectДокумент18 страницMechanical Completion Procedure for HPCL Visakh ProjectLegend AnbuОценок пока нет
- Valves 101: Gobind KhianiДокумент56 страницValves 101: Gobind Khianikongara_inst1118Оценок пока нет
- วิธีคำนวน activated carbon PDFДокумент7 страницวิธีคำนวน activated carbon PDFPépé TechopathamОценок пока нет
- Unit 3 Steam GenerationДокумент30 страницUnit 3 Steam GenerationkhalimnОценок пока нет
- Explosion at The Conoco Humber Refinery - Lessons Learned PDFДокумент29 страницExplosion at The Conoco Humber Refinery - Lessons Learned PDFMuhammad IqmalОценок пока нет
- Presentasi - Cortec CGIДокумент38 страницPresentasi - Cortec CGImoch ardiansyahОценок пока нет
- Coke Drum Remaining LifeДокумент4 страницыCoke Drum Remaining Lifeash1968Оценок пока нет
- Blind List C101 ReactorДокумент2 страницыBlind List C101 ReactorMadhan KannanОценок пока нет
- Sanchit Kapil (CV)Документ4 страницыSanchit Kapil (CV)Sanchit KapilОценок пока нет
- Main Fractionator Water Wash Systems PTQ REVAMPS 2006 PDFДокумент5 страницMain Fractionator Water Wash Systems PTQ REVAMPS 2006 PDFmajope1966Оценок пока нет
- BubbleCap Distillation Manuals - FINAL 29082018 - 17PgsДокумент17 страницBubbleCap Distillation Manuals - FINAL 29082018 - 17PgsSagar MorjeОценок пока нет
- Introduction To Uop: Jim Mcgehee Development Specialist, Heavy OilsДокумент22 страницыIntroduction To Uop: Jim Mcgehee Development Specialist, Heavy OilsAnkush BhandariОценок пока нет
- OM HandbookДокумент163 страницыOM HandbookAmanullahОценок пока нет
- GP 06-25 - Design For The PrevДокумент24 страницыGP 06-25 - Design For The Prev1339979Оценок пока нет
- BP GS162-1 Valves PDFДокумент24 страницыBP GS162-1 Valves PDFMohd Khairul100% (1)
- Drum in BoilerДокумент18 страницDrum in BoilerRuban Kumar100% (1)
- File-Chemical InjectДокумент58 страницFile-Chemical InjectEnvОценок пока нет
- Investigation of Platformer Reactor Nozzle CrackingДокумент12 страницInvestigation of Platformer Reactor Nozzle CrackingMubeenОценок пока нет
- Coke Drum DesignДокумент6 страницCoke Drum Designkutts76Оценок пока нет
- Saes L 140 PDFДокумент13 страницSaes L 140 PDFsamsurendran_mech4020Оценок пока нет
- Delayed Coker Blowdown System Water Reuse Moloney ExxonMobil DCU Budapest 2017Документ23 страницыDelayed Coker Blowdown System Water Reuse Moloney ExxonMobil DCU Budapest 2017Obrejan CosminОценок пока нет
- Hydraulic Decoking System: Nnovation Efficiency QualityДокумент8 страницHydraulic Decoking System: Nnovation Efficiency QualitykennymagallanesОценок пока нет
- 09 Piping Fittings and Valves - TeddyДокумент9 страниц09 Piping Fittings and Valves - TeddyoctatheweelОценок пока нет
- 01 Saip 38Документ14 страниц01 Saip 38Arjun RawatОценок пока нет
- Tail Gas Treatment Unit Facility Inspection ReportДокумент7 страницTail Gas Treatment Unit Facility Inspection Reportabdelkader benabdallahОценок пока нет
- SRU Turnaround Monitoring ReportДокумент6 страницSRU Turnaround Monitoring ReportAllan BadilloОценок пока нет
- Jif 20 Van 014 Fat Qad 2419 Fat ShelterДокумент10 страницJif 20 Van 014 Fat Qad 2419 Fat Shelteransalkr_6232335Оценок пока нет
- Leakage Acceptance Rates Comparison Metal & Soft Seated Valves Api 598/api 6D/Mss Sp-61/Fci 70-2Документ5 страницLeakage Acceptance Rates Comparison Metal & Soft Seated Valves Api 598/api 6D/Mss Sp-61/Fci 70-2Ashfaq AnwerОценок пока нет
- Condenser and Cooler Inspection ReportsДокумент6 страницCondenser and Cooler Inspection ReportsSampatОценок пока нет
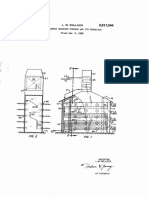
- Dec. 15, 1959 L. W. Pollock 2,917,564: Hydrocarbon Cracking Furnace and Its Operation Filed Jan. 5, 1959Документ6 страницDec. 15, 1959 L. W. Pollock 2,917,564: Hydrocarbon Cracking Furnace and Its Operation Filed Jan. 5, 1959regina pramuditaОценок пока нет
- Hazop StudyДокумент19 страницHazop StudyARSAL HASHMIОценок пока нет
- Deviation Sheet On Standard Quality Plan: Project Package Manufacturer Item Name SQP NoДокумент5 страницDeviation Sheet On Standard Quality Plan: Project Package Manufacturer Item Name SQP NoSuraj ShettyОценок пока нет
- BASF - Hose Inspection Frequency TableДокумент1 страницаBASF - Hose Inspection Frequency Tablepablo fornesОценок пока нет
- Salman Offshore Facilities Laybarge Welding SpecificationДокумент45 страницSalman Offshore Facilities Laybarge Welding SpecificationLit Phen TuОценок пока нет
- The Hot Bypass Pressure Control Rev. Agosto 2018Документ12 страницThe Hot Bypass Pressure Control Rev. Agosto 2018luiz.henriqueОценок пока нет
- Potential Damage PKTДокумент7 страницPotential Damage PKTFebri Ramdani NugrahaОценок пока нет
- Corrosion of Steels in Sour Gas EnvironmentДокумент179 страницCorrosion of Steels in Sour Gas Environmentaathittaya100% (1)
- 50 Chemical Injection System Access Fitting Assemblies - 50-DS Revc PDFДокумент19 страниц50 Chemical Injection System Access Fitting Assemblies - 50-DS Revc PDFChemkhiОценок пока нет
- 1.structured Packing PresentationДокумент27 страниц1.structured Packing PresentationRavindra V. LakhapatiОценок пока нет
- Sabp A 001Документ22 страницыSabp A 001kuse2456Оценок пока нет
- Human Factors in Process Plant Operation by David A. StrobharДокумент66 страницHuman Factors in Process Plant Operation by David A. StrobharAbdelsalam MahmoudОценок пока нет
- 05 V PattabathulaДокумент16 страниц05 V Pattabathulapcorreia_81Оценок пока нет
- WSAC Alternative To CWДокумент47 страницWSAC Alternative To CWweweqweqwОценок пока нет
- Basic Mechanical-ReqrmntДокумент14 страницBasic Mechanical-Reqrmntadel rihanaОценок пока нет
- Piper Alpha Background & ShortcomingsДокумент4 страницыPiper Alpha Background & Shortcomingsfashwin0% (1)
- Pipe Rupture and Fire: Group 07 Case Study ReportДокумент7 страницPipe Rupture and Fire: Group 07 Case Study Reportsukanta60Оценок пока нет
- Husky FireДокумент2 страницыHusky Firevijayi dhansarОценок пока нет
- Feyzin Oil Refinery DisasterДокумент8 страницFeyzin Oil Refinery DisasterDavid Alonso Cedano EchevarriaОценок пока нет
- Feyzin DisasterДокумент4 страницыFeyzin Disastermichaelalex1001100% (3)
- Epcsm Term PaperДокумент13 страницEpcsm Term PaperFake accОценок пока нет
- Machine Design TEList Spring 2016Документ3 страницыMachine Design TEList Spring 2016Reynald De VeraОценок пока нет
- Engineering Materials and Metallurgy Notes PDFДокумент0 страницEngineering Materials and Metallurgy Notes PDFSenthilkumar Subbiah50% (2)
- Design ModelДокумент1 страницаDesign ModelReynald De VeraОценок пока нет
- Chpater 1 - Rev2Документ26 страницChpater 1 - Rev2Reynald De VeraОценок пока нет
- Appndx74 Model Selection by RCP2 GripperДокумент1 страницаAppndx74 Model Selection by RCP2 GripperReynald De VeraОценок пока нет
- Guideline Study ProjectДокумент2 страницыGuideline Study ProjectReynald De VeraОценок пока нет
- Games 2Документ1 страницаGames 2Reynald De VeraОценок пока нет
- Advanced CalculusДокумент592 страницыAdvanced Calculusjosemarcelod7088Оценок пока нет
- Teacher Manual R3Документ54 страницыTeacher Manual R3George KaridisОценок пока нет
- Games 1Документ1 страницаGames 1Reynald De VeraОценок пока нет
- Floor Polisher: Operating Instructions (ENG)Документ35 страницFloor Polisher: Operating Instructions (ENG)Reynald De VeraОценок пока нет
- Manually Operated Direct Seeding Rice Planter MachineДокумент2 страницыManually Operated Direct Seeding Rice Planter MachineReynald De VeraОценок пока нет
- Life Cycle Assessment of Floor Care: A Comparative Study of The Twister™ Method and Floor Care Methods Using Polish and WaxДокумент7 страницLife Cycle Assessment of Floor Care: A Comparative Study of The Twister™ Method and Floor Care Methods Using Polish and WaxReynald De VeraОценок пока нет
- Floor Polisher: Operating Instructions (ENG)Документ35 страницFloor Polisher: Operating Instructions (ENG)Reynald De VeraОценок пока нет
- Appndx74 Model Selection by RCP2 GripperДокумент1 страницаAppndx74 Model Selection by RCP2 GripperReynald De VeraОценок пока нет
- PolymersДокумент1 страницаPolymersReynald De VeraОценок пока нет
- Duct Sizing and HVAC CalculationДокумент21 страницаDuct Sizing and HVAC Calculationsardarmkhan80% (5)
- SpongeДокумент1 страницаSpongeReynald De VeraОценок пока нет
- SpongeДокумент1 страницаSpongeReynald De VeraОценок пока нет
- SpongeДокумент1 страницаSpongeReynald De VeraОценок пока нет
- Chevron Regulatory Report Draft For Public CommentДокумент115 страницChevron Regulatory Report Draft For Public CommentKQED NewsОценок пока нет
- Chevron Richmond Refinery Pipe Rupture and Fire PDFДокумент7 страницChevron Richmond Refinery Pipe Rupture and Fire PDFReynald De VeraОценок пока нет
- Kory Judd IntroductionДокумент1 страницаKory Judd IntroductionHoang NamОценок пока нет
- Hydrocracking catalyst developments for improved activity and selectivityДокумент7 страницHydrocracking catalyst developments for improved activity and selectivityLindsey BondОценок пока нет
- Chevron Richmond Refinery Revised Renewal Project - Conditional Use Permit/Amended EIR ApplicationДокумент20 страницChevron Richmond Refinery Revised Renewal Project - Conditional Use Permit/Amended EIR ApplicationCVX_Richmond_RenewalОценок пока нет
- Chevron Final Investigation Report 2015-01-28Документ132 страницыChevron Final Investigation Report 2015-01-28Riccardo CozzaОценок пока нет
- RefineriesДокумент273 страницыRefineriesLuis Santos100% (1)
- Materials Selection Challenges in The Refining Industry Dave CookeДокумент26 страницMaterials Selection Challenges in The Refining Industry Dave CookeAlaeddin Guner RodopОценок пока нет
- CSB Investigation of Chevron Refinery Pipe Rupture and FireДокумент5 страницCSB Investigation of Chevron Refinery Pipe Rupture and Firesukanta60Оценок пока нет
- Chevron Interim Report Final 2013-04-17 PDFДокумент70 страницChevron Interim Report Final 2013-04-17 PDFYuvaraj NithyanandamОценок пока нет
- Chemical Safety Board Investigates Chevron Refinery Fire - Chemical & Engineering NewsДокумент4 страницыChemical Safety Board Investigates Chevron Refinery Fire - Chemical & Engineering NewsFatemeh MehrbakhshОценок пока нет
- Lack of Mechanical Integrity Blamed For Leak at Exxon Mobil RefineryДокумент4 страницыLack of Mechanical Integrity Blamed For Leak at Exxon Mobil RefineryKalaivani ArunachalamОценок пока нет