Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Diarrhoea Master Final 2011Документ43 страницыDiarrhoea Master Final 2011Gunaseelan KumarОценок пока нет
- STG PediatricДокумент314 страницSTG PediatricVitalis Mbuya50% (2)
- Reading Sub-Test: Part AДокумент18 страницReading Sub-Test: Part Amarine gns71% (7)
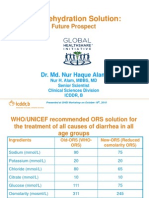
- Oral Rehydration Solution:: Future ProspectДокумент48 страницOral Rehydration Solution:: Future ProspectmustikaarumОценок пока нет
- (Living High and Letting Die) - Peter - UngerДокумент172 страницы(Living High and Letting Die) - Peter - UngerHean HeanОценок пока нет
- Nutrient Timing and Training: The Warfighter Nutrition GuideДокумент15 страницNutrient Timing and Training: The Warfighter Nutrition GuideBenОценок пока нет
- Management of CholeraДокумент69 страницManagement of CholeraNatalia LawrenceОценок пока нет
- CPG AID - Pocket Guide.v7 PDFДокумент31 страницаCPG AID - Pocket Guide.v7 PDFR ParkОценок пока нет
- Dirhea and IBSДокумент6 страницDirhea and IBSDavid HosamОценок пока нет
- Acute Diarrhoea PhysiopatologyДокумент3 страницыAcute Diarrhoea PhysiopatologyFabiana TorresОценок пока нет
- Post Lab Experiment 11 13 PDFДокумент4 страницыPost Lab Experiment 11 13 PDFDekdek MendozaОценок пока нет
- Thermal Work Limit-Working Zones: Control Interventions, Rest-Work and Rehydration SchedulesДокумент1 страницаThermal Work Limit-Working Zones: Control Interventions, Rest-Work and Rehydration SchedulesSuprkliОценок пока нет
- Drug Study Ciprofloxacin QuinosynДокумент10 страницDrug Study Ciprofloxacin QuinosynNelle ReyОценок пока нет
- Maintaining Fluid & Electrolyte Balance in The BodyДокумент124 страницыMaintaining Fluid & Electrolyte Balance in The BodyKingJayson Pacman06100% (1)
- Pharma - Drugs Affecting Git MotilityДокумент6 страницPharma - Drugs Affecting Git MotilityBobet ReñaОценок пока нет
- Diarrhea Noxious Toxic Loose: Oral Rehydration SolutionsДокумент48 страницDiarrhea Noxious Toxic Loose: Oral Rehydration SolutionsShane ShopeeОценок пока нет
- ORSДокумент11 страницORSrrahulpatelОценок пока нет
- Ethiopian Drug IndexДокумент71 страницаEthiopian Drug IndexYoussef KaidОценок пока нет
- Diagnosis and Management of Dehydration in ChildrenДокумент5 страницDiagnosis and Management of Dehydration in ChildrenCitlalli MorenoОценок пока нет
- Dehydration - PedsCase - v9Документ1 страницаDehydration - PedsCase - v9Chinenye ModestaОценок пока нет
- DR Perla D Santos OcampoДокумент2 страницыDR Perla D Santos OcampoAiza CabolesОценок пока нет
- Acute Viral Gastroenteritis in Children in Resource-Rich Countries: Management and PreventionДокумент25 страницAcute Viral Gastroenteritis in Children in Resource-Rich Countries: Management and Preventiondaniso12Оценок пока нет
- Pediatrics-in-Review 1989 - Acute Diarrhea in Children PDFДокумент10 страницPediatrics-in-Review 1989 - Acute Diarrhea in Children PDFmob3Оценок пока нет
- Bronchiolitis Case StudyДокумент14 страницBronchiolitis Case StudyTey Herrera0% (1)
- Oral Rehydration SaltДокумент3 страницыOral Rehydration SaltVincent ManganaanОценок пока нет
- Electrolyte Replacement - Critical Care ICU/PCU (30400716)Документ7 страницElectrolyte Replacement - Critical Care ICU/PCU (30400716)Lubna AliОценок пока нет
- Essential Drug ListДокумент40 страницEssential Drug ListSuresh DhunganaОценок пока нет
- Diarrhea FlipchartДокумент27 страницDiarrhea FlipchartEliana SochaОценок пока нет
- Fluid Treatment Pattern VSДокумент8 страницFluid Treatment Pattern VSDen PeraОценок пока нет
- Skenario C Blok 15 Tahun 2018Документ5 страницSkenario C Blok 15 Tahun 2018Nur akilaОценок пока нет