Вам также может понравиться
- Emergency Severity IndexДокумент114 страницEmergency Severity Indexpafin100% (3)
- Health History AssignmentДокумент6 страницHealth History AssignmentgeegundelyОценок пока нет
- Bridenbaughs Blockade Clinical Anesthesia Medicine 0781773881Документ4 страницыBridenbaughs Blockade Clinical Anesthesia Medicine 0781773881docbin0% (2)
- APARQ QuestionnaireДокумент6 страницAPARQ QuestionnairehumanismeОценок пока нет
- NCP For AnaphylacticДокумент3 страницыNCP For AnaphylacticRommar Romero67% (3)
- Journal M 11Документ8 страницJournal M 11Pit PitoyoОценок пока нет
- A Clinical Study of Programmed Labour and Its Maternal and Foetal OutcomeДокумент4 страницыA Clinical Study of Programmed Labour and Its Maternal and Foetal OutcomeInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Deep Breathing Techniques Relieve Labor PainДокумент6 страницDeep Breathing Techniques Relieve Labor PainMuthya GhitaОценок пока нет
- Neetu, Poonam Sheoran, Rashmi PanchalДокумент6 страницNeetu, Poonam Sheoran, Rashmi PanchalMuzdalifah Karina DMОценок пока нет
- Uprak Rubrik Bu IzfaaizahДокумент12 страницUprak Rubrik Bu IzfaaizahMaya Ulfah apriliyaОценок пока нет
- Meta 2Документ20 страницMeta 2fhie_amandaОценок пока нет
- Effects of Yoga Relaxation On Anxiety Levels Among Pregnant Women-DikonversiДокумент10 страницEffects of Yoga Relaxation On Anxiety Levels Among Pregnant Women-DikonversimayaОценок пока нет
- Jurnal Kespro InggrisДокумент11 страницJurnal Kespro InggrisFarah RahОценок пока нет
- Postnatal Exercises Improve Quality of LifeДокумент4 страницыPostnatal Exercises Improve Quality of LiferohiniОценок пока нет
- International Journal of Health Sciences and ResearchДокумент9 страницInternational Journal of Health Sciences and ResearchAnnisa MeilaniОценок пока нет
- Jurnal Post PartumДокумент11 страницJurnal Post PartumjayaОценок пока нет
- Hartati 2019 J. Phys. Conf. Ser. 1351 012091Документ7 страницHartati 2019 J. Phys. Conf. Ser. 1351 012091Derison MarsinovaОценок пока нет
- J. Appl. Environ. Biol. Sci., 8 (3) 51-59, 2018 PDFДокумент9 страницJ. Appl. Environ. Biol. Sci., 8 (3) 51-59, 2018 PDFDian Septi WidowatiОценок пока нет
- Content ServerДокумент9 страницContent ServerJohn SteplОценок пока нет
- The Effect of DismenorhoeДокумент18 страницThe Effect of DismenorhoeNarmin FaisalОценок пока нет
- RCT Zumba ExerciseДокумент5 страницRCT Zumba ExerciseSukmarahayuОценок пока нет
- Nop2 8 2345Документ9 страницNop2 8 2345api-600421611Оценок пока нет
- 1098 2116 1 SM PDFДокумент9 страниц1098 2116 1 SM PDFAnjar Mac TravizzОценок пока нет
- 5615 23222 1 PBДокумент4 страницы5615 23222 1 PBIca IsmailОценок пока нет
- The Effect of Progressive Muscle Relaxation On PosДокумент16 страницThe Effect of Progressive Muscle Relaxation On PosLaelannie MagpayoОценок пока нет
- Wa0008. PDFДокумент12 страницWa0008. PDFLal NandaniОценок пока нет
- Ibu NifasДокумент6 страницIbu NifasNazwan Adwa NabilahОценок пока нет
- 21Документ7 страниц21Sandy ApriОценок пока нет
- 7 6325-18262-1-PB (Scholar) AcupresurДокумент5 страниц7 6325-18262-1-PB (Scholar) Acupresur201702075Nur Vika Indah SariОценок пока нет
- The Effects of Prenatal Yoga On The Outcomes of Labor and DeliveryДокумент16 страницThe Effects of Prenatal Yoga On The Outcomes of Labor and Deliveryapi-621758677Оценок пока нет
- Complementary Therapies in Clinical Practice: Semiha Ayd In Özkan, Gülay Rath FischДокумент6 страницComplementary Therapies in Clinical Practice: Semiha Ayd In Özkan, Gülay Rath FischAlek OkeОценок пока нет
- Effectiveness of Breathing Exercise On Reducing Pain Perception and State Anxiety Among Primi ParturientsДокумент8 страницEffectiveness of Breathing Exercise On Reducing Pain Perception and State Anxiety Among Primi ParturientsPutra SpОценок пока нет
- 1Документ6 страниц1elda zulkarnainОценок пока нет
- Asian Nursing Research: - Ilknur G Oks In, Sultan Ayaz-AlkayaДокумент6 страницAsian Nursing Research: - Ilknur G Oks In, Sultan Ayaz-AlkayaBella ShintaОценок пока нет
- Pi Is 1976131717304267Документ5 страницPi Is 1976131717304267Yenie YenОценок пока нет
- Jurnal Five FingerДокумент10 страницJurnal Five FingerYunita AmiliaОценок пока нет
- Musikterapi RannysyahfiraДокумент69 страницMusikterapi RannysyahfiraRanny SyahfiraОценок пока нет
- Jurnal Musik InternasionalДокумент6 страницJurnal Musik InternasionalBwana KuroiОценок пока нет
- Review of LiteratureДокумент16 страницReview of Literatureakhils.igjОценок пока нет
- Evaluation of The 'Healthy Start To Pregnancy' Early Antenatal Health Promotion Workshop: A Randomized Controlled TrialДокумент12 страницEvaluation of The 'Healthy Start To Pregnancy' Early Antenatal Health Promotion Workshop: A Randomized Controlled TrialErfann Yuda AnsyariОценок пока нет
- Nursing Care Reduces Labor Pain and CostsДокумент14 страницNursing Care Reduces Labor Pain and Costssgd bsepuluhОценок пока нет
- RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES M.SC NURSING DISSERTATION ON EFFECTIVENESS OF PROGRESSIVE MUSCLE RELAXATION TECHNIQUE ON PAINДокумент18 страницRAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES M.SC NURSING DISSERTATION ON EFFECTIVENESS OF PROGRESSIVE MUSCLE RELAXATION TECHNIQUE ON PAINRofidaUpitОценок пока нет
- Measuring Stress in Mothers of High-Risk Babies and the Effectiveness of Relaxation TechniquesДокумент6 страницMeasuring Stress in Mothers of High-Risk Babies and the Effectiveness of Relaxation Techniquesmini joyОценок пока нет
- DIT SoniyaMДокумент6 страницDIT SoniyaMBella FebriantiОценок пока нет
- ABSTRACT ItismitaДокумент4 страницыABSTRACT ItismitaPabhat KumarОценок пока нет
- Effect of Birth Ball On Labor Pain Relief A Systematic ReviewДокумент8 страницEffect of Birth Ball On Labor Pain Relief A Systematic Reviewgina hardiatiОценок пока нет
- Assignment On ": Annotated Bibliography"Документ4 страницыAssignment On ": Annotated Bibliography"Deepti KukretiОценок пока нет
- San Vera Materi AДокумент13 страницSan Vera Materi Aendah desfindaОценок пока нет
- Comparative Effect of Nature-Based Sounds Intervention and Headphones Intervention On Pain Severity After Cesarean SectionДокумент11 страницComparative Effect of Nature-Based Sounds Intervention and Headphones Intervention On Pain Severity After Cesarean SectionDwi AndayaniОценок пока нет
- Pengaruh L14 Terhadap Peningkatan Kontraksi Pada Kala I PersalinanДокумент6 страницPengaruh L14 Terhadap Peningkatan Kontraksi Pada Kala I PersalinanKiki ElvianiОценок пока нет
- 264 496 1 SM PDFДокумент5 страниц264 496 1 SM PDFVina DaniatiОценок пока нет
- Jurnal Kenaikan Berat Badan WhinikeДокумент10 страницJurnal Kenaikan Berat Badan WhinikeWhinike CintyaОценок пока нет
- Synthesis Paper - Final DraftДокумент15 страницSynthesis Paper - Final Draftapi-469407326Оценок пока нет
- AmornlertДокумент5 страницAmornlerttmc20Оценок пока нет
- Clinical StudyДокумент8 страницClinical StudyFatimatus ZahroОценок пока нет
- Assessing Effectiveness of Warm Compress on Labour PainДокумент21 страницаAssessing Effectiveness of Warm Compress on Labour PainHanny Novianti100% (2)
- Effects of LI-4 and SP-6 Acupuncture On Labor Pain, Cortisol Level and Duration of LaborДокумент6 страницEffects of LI-4 and SP-6 Acupuncture On Labor Pain, Cortisol Level and Duration of LaborJonasMarçaloОценок пока нет
- Effect of Therapeutic Massage On Relieving Pregnancy DiscomfortsДокумент8 страницEffect of Therapeutic Massage On Relieving Pregnancy DiscomfortsDerison MarsinovaОценок пока нет
- 1098 2116 1 SMДокумент9 страниц1098 2116 1 SMerryОценок пока нет
- The Effect of Giving Dark Chocolate On Primary Dismenorrhorea in Junior High School Students in Long Ikis District, Pader Regency Year 2022Документ7 страницThe Effect of Giving Dark Chocolate On Primary Dismenorrhorea in Junior High School Students in Long Ikis District, Pader Regency Year 2022International Journal of Innovative Science and Research TechnologyОценок пока нет
- Research Article: Kasturba Gandhi Nursing CollegeДокумент5 страницResearch Article: Kasturba Gandhi Nursing CollegesanthiyasandyОценок пока нет
- Picot ProposalДокумент6 страницPicot Proposalapi-282602935100% (3)
- Physical Therapy For BeginnersДокумент4 страницыPhysical Therapy For BeginnersBogart MacatangayОценок пока нет
- Literature Review On DysmenorrhoeaДокумент4 страницыLiterature Review On Dysmenorrhoeaafdtsxuep100% (1)
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsОт EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsОценок пока нет
- Vaksin VarelaДокумент8 страницVaksin VarelaPutra EkaОценок пока нет
- KemoДокумент11 страницKemoPutra EkaОценок пока нет
- NutritionsДокумент9 страницNutritionsPutra EkaОценок пока нет
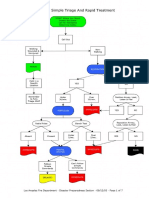
- Acute Pulmonary Edema Algorithm: Consider ConsultationДокумент1 страницаAcute Pulmonary Edema Algorithm: Consider ConsultationPutra EkaОценок пока нет
- Sample WordДокумент1 страницаSample WordNuno AlvesОценок пока нет
- Jurnal FixДокумент6 страницJurnal FixPutra EkaОценок пока нет
- Causes and Treatment of Pulmonary EdemaДокумент1 страницаCauses and Treatment of Pulmonary EdemaShila Wisnasari100% (2)
- Hominid EvolutionДокумент2 страницыHominid EvolutionJosephine TorresОценок пока нет
- Maternitas JurnalДокумент12 страницMaternitas JurnalPutra EkaОценок пока нет
- Jurnal FixДокумент6 страницJurnal FixPutra EkaОценок пока нет
- Clean Vs Sterile Dressing Techniques For.7Документ5 страницClean Vs Sterile Dressing Techniques For.7Putra EkaОценок пока нет
- Start TriageДокумент7 страницStart TriagePutra EkaОценок пока нет
- 4686216Документ3 страницы4686216Putra EkaОценок пока нет
- BasicДокумент8 страницBasicPutra EkaОценок пока нет
- Ipi 107451Документ5 страницIpi 107451Ade Churie TanjayaОценок пока нет
- RoleДокумент8 страницRolePutra EkaОценок пока нет
- BasicДокумент8 страницBasicPutra EkaОценок пока нет
- 4686216Документ3 страницы4686216Putra EkaОценок пока нет
- TriageДокумент6 страницTriagePutra EkaОценок пока нет
- BasicДокумент8 страницBasicPutra EkaОценок пока нет
- F60 Turbine Operator Manual PDFДокумент130 страницF60 Turbine Operator Manual PDFNoel SamОценок пока нет
- Government Medical College, Jammu: Public AppealДокумент3 страницыGovernment Medical College, Jammu: Public AppealJOATОценок пока нет
- CSF Dynamics in Dandy-Walker Syndrome ExplainedДокумент5 страницCSF Dynamics in Dandy-Walker Syndrome ExplainedSergio SaraivaОценок пока нет
- Analgesia Epidural Current Views and ApproachesДокумент168 страницAnalgesia Epidural Current Views and ApproachesManuel Ortega100% (2)
- PURE YANG' AND 'YOUNG YIN AND YANG' IN PEDIATRICSДокумент33 страницыPURE YANG' AND 'YOUNG YIN AND YANG' IN PEDIATRICSRamesh Babu ManivannanОценок пока нет
- Folder Flexya Ita Pag AffiancateДокумент2 страницыFolder Flexya Ita Pag AffiancateemikyОценок пока нет
- Carriere® SLX Patient EducationДокумент2 страницыCarriere® SLX Patient EducationOrtho OrganizersОценок пока нет
- Pharyngitis: John C. Arnold and Victor NizetДокумент10 страницPharyngitis: John C. Arnold and Victor NizetPratita Jati PermatasariОценок пока нет
- List of Hospitals in Ahmedabad DistrictДокумент190 страницList of Hospitals in Ahmedabad DistrictTushar Y. JaniОценок пока нет
- Revision Surgery in Otolaryngology: Book and Multimedia ReviewsДокумент2 страницыRevision Surgery in Otolaryngology: Book and Multimedia ReviewsBrînduşa CiobanuОценок пока нет
- Apex LocatorsДокумент6 страницApex LocatorsbanupriyamdsОценок пока нет
- Neuromotor and Cognitive Functions in 4Документ60 страницNeuromotor and Cognitive Functions in 4ARICEL SALDIVIAОценок пока нет
- Myresume 1Документ3 страницыMyresume 1MusadunDunОценок пока нет
- PLM 12399a Product Information Rad G Continuous British PDFДокумент2 страницыPLM 12399a Product Information Rad G Continuous British PDFAlina Vitali TabarceaОценок пока нет
- Epistatus Administer DerbyPCT PDFДокумент2 страницыEpistatus Administer DerbyPCT PDFAlex GeorgeОценок пока нет
- New Intern Guide Quick NotesДокумент8 страницNew Intern Guide Quick NotesTrisОценок пока нет
- PsychologyДокумент4 страницыPsychologySushmita SahuОценок пока нет
- Medical TerminologyДокумент27 страницMedical TerminologyXuan CarpentierОценок пока нет
- Madhya Pradesh Medical Science University, Jabalpur (M.P.)Документ78 страницMadhya Pradesh Medical Science University, Jabalpur (M.P.)Vinay Mishra100% (1)
- AMA SpecialtyByTOPS 12-9-10Документ10 страницAMA SpecialtyByTOPS 12-9-10bmartindoyle6396Оценок пока нет
- Inguinal HerniaДокумент27 страницInguinal HerniaNeneng WulandariОценок пока нет
- Radiological Signs (Shënja Radiologjike) - 5Документ112 страницRadiological Signs (Shënja Radiologjike) - 5Sllavko K. KallfaОценок пока нет
- Anaesthesia & Intensive Care Medicine Volume 11 Issue 4 2010 (Doi 10.1016/j.mpaic.2009.12.013) Ben Shelley Nick Sutcliffe - Total Intravenous AnaesthesiaДокумент3 страницыAnaesthesia & Intensive Care Medicine Volume 11 Issue 4 2010 (Doi 10.1016/j.mpaic.2009.12.013) Ben Shelley Nick Sutcliffe - Total Intravenous AnaesthesiamikhatiarОценок пока нет
- Practice Set 1Документ5 страницPractice Set 1AMAN BISWASОценок пока нет
- Cep2020 Chapter03c HealthДокумент10 страницCep2020 Chapter03c HealthLyan TejedoОценок пока нет
- Biomechanics of The ElbowДокумент16 страницBiomechanics of The ElbowAsmaa Ahmad SharawyОценок пока нет
- Snake BiteДокумент18 страницSnake BiteRejana JonesОценок пока нет