Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Highland Guidelines - LDK 2013-2-15Документ3 страницыHighland Guidelines - LDK 2013-2-15andrew herringОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- AclsДокумент20 страницAclsqueennita69100% (4)
- K Opiods For Pain BupДокумент2 страницыK Opiods For Pain Bupandrew herringОценок пока нет
- Natural Anxiety CuresДокумент93 страницыNatural Anxiety Curesd_probst5098100% (1)
- Roux 2013Документ7 страницRoux 2013andrew herringОценок пока нет
- Buprenorphine 2016-7-18Документ1 страницаBuprenorphine 2016-7-18andrew herringОценок пока нет
- Original Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve BlockДокумент7 страницOriginal Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve Blockandrew herringОценок пока нет
- Rib Fracture W: PecsДокумент8 страницRib Fracture W: Pecsandrew herring100% (1)
- Rib Fracture SerratusДокумент3 страницыRib Fracture Serratusandrew herring100% (1)
- Ultrasound-Guided Block of TheДокумент6 страницUltrasound-Guided Block of Theandrew herringОценок пока нет
- Intravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-OperatóriaДокумент6 страницIntravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-Operatóriaandrew herringОценок пока нет
- Herring ED Intractable Abdominal pain-N+VДокумент1 страницаHerring ED Intractable Abdominal pain-N+Vandrew herringОценок пока нет
- 3.2.16.highland Emergency Medicine Journal Club Methods.2Документ2 страницы3.2.16.highland Emergency Medicine Journal Club Methods.2andrew herringОценок пока нет
- Ketamine As Rescue Treatment FДокумент8 страницKetamine As Rescue Treatment Fandrew herringОценок пока нет
- Dex For Dental Pain & SwellingДокумент7 страницDex For Dental Pain & Swellingandrew herring100% (1)
- Nej MR A 1511480Документ9 страницNej MR A 1511480Tohari Masidi AminОценок пока нет
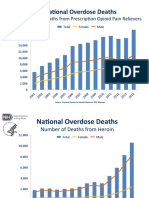
- OPR - Heroin DeathsДокумент2 страницыOPR - Heroin Deathsandrew herringОценок пока нет
- CVS Action Plan v2Документ1 страницаCVS Action Plan v2andrew herringОценок пока нет
- Ultrasound Guided Interventional Procedures In.13Документ14 страницUltrasound Guided Interventional Procedures In.13andrew herring100% (1)
- Ultrasound Guided Interventional Procedures In.4Документ13 страницUltrasound Guided Interventional Procedures In.4andrew herringОценок пока нет
- Special Articles: Awake Intubation Intubation After Induction of General AnesthesiaДокумент1 страницаSpecial Articles: Awake Intubation Intubation After Induction of General AnesthesiaOKE channelОценок пока нет
- CHEMOTHERAPYДокумент28 страницCHEMOTHERAPYDwi CahyaОценок пока нет
- Fast Hugs MaidenДокумент8 страницFast Hugs MaidenPriscila Navarro MedinaОценок пока нет
- MHS 6401Документ5 страницMHS 6401Delelegn EmwodewОценок пока нет
- Does Klonopin (Clonazepam) Work For MigrainesДокумент4 страницыDoes Klonopin (Clonazepam) Work For MigrainesTooba SiddiquiОценок пока нет
- Paediatric Drug DosingДокумент18 страницPaediatric Drug DosingDR JAMAL WARISОценок пока нет
- America Stock Viernes 01-07-2022Документ41 страницаAmerica Stock Viernes 01-07-2022Rosa Irma GaunaОценок пока нет
- Treatment of Schizophrenia and Management of Drug SideДокумент83 страницыTreatment of Schizophrenia and Management of Drug SideAbelОценок пока нет
- Sample NURSING PROCESS IN PHARMACOLOGY PDFДокумент7 страницSample NURSING PROCESS IN PHARMACOLOGY PDFVic Intia PaaОценок пока нет
- 2020 Conference PaperДокумент2 страницы2020 Conference PaperHealthcare Pro LearningОценок пока нет
- Clinical Pharmacology of Antibiotics - PMCДокумент19 страницClinical Pharmacology of Antibiotics - PMCJosette LeyvaОценок пока нет
- Antibiotic Cross-Sensitivity ChartДокумент1 страницаAntibiotic Cross-Sensitivity ChartChing JuОценок пока нет
- IMN1207 McGillActiveProtocolsДокумент11 страницIMN1207 McGillActiveProtocolsapi-3714923Оценок пока нет
- Med GuideДокумент7 страницMed GuideEko YuliantoОценок пока нет
- AclsДокумент2 страницыAclsEman ElzeftawyОценок пока нет
- Pricelist ErelaДокумент1 страницаPricelist ErelaMutia FarmaОценок пока нет
- 11.drug StudyДокумент1 страница11.drug StudyFreisanChenMandumotanОценок пока нет
- Emergency Responder Bag: QTY Unit Item Name Intubation SetДокумент3 страницыEmergency Responder Bag: QTY Unit Item Name Intubation SetferdyОценок пока нет
- Chapter 15 Treatment of Psychological DisordersДокумент52 страницыChapter 15 Treatment of Psychological DisordersChehekОценок пока нет
- HOSPITAL Past PapersДокумент6 страницHOSPITAL Past PapersMr nobodyОценок пока нет
- Az Essential RX ListДокумент141 страницаAz Essential RX ListAbdullah HamdanОценок пока нет
- Rusan Pharma Product ListДокумент4 страницыRusan Pharma Product ListSanjay SharmaОценок пока нет
- Meet 4. Penyiapan Obat SitostatikaДокумент47 страницMeet 4. Penyiapan Obat SitostatikaChoirun NisaОценок пока нет
- One Compartment Open Model IV Bolus: DR Mohammad IssaДокумент79 страницOne Compartment Open Model IV Bolus: DR Mohammad IssaPronoy SahaОценок пока нет
- Alevo Alkem (Ulticare) (Levofloxacin) : Strength Presentation PriceДокумент21 страницаAlevo Alkem (Ulticare) (Levofloxacin) : Strength Presentation Pricepathan mohidОценок пока нет
- MCHДокумент21 страницаMCHmoubarkОценок пока нет
- Strategy Increase SellДокумент7 страницStrategy Increase SellPrashun Shekhar SrivastavaОценок пока нет
- 2018 I.V. Push Administration of Medications Reconstituted With 0.9% NSДокумент2 страницы2018 I.V. Push Administration of Medications Reconstituted With 0.9% NSDaniela MéndezОценок пока нет