Вам также может понравиться
- Career Opportunities For MBBS Doctors On Contract Basis Udate 21-2-2017Документ2 страницыCareer Opportunities For MBBS Doctors On Contract Basis Udate 21-2-2017malik003Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- VascularDisordersLiver2009 PDFДокумент36 страницVascularDisordersLiver2009 PDFmalik003Оценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Recent Advances in The Development of Anti-Tuberculosis Drugs Acting On Multidrug-Resistant Strains: A ReviewДокумент18 страницRecent Advances in The Development of Anti-Tuberculosis Drugs Acting On Multidrug-Resistant Strains: A Reviewmalik003Оценок пока нет
- History in Ob/Gy: Ahmed AbdulwahabДокумент9 страницHistory in Ob/Gy: Ahmed Abdulwahabmalik003Оценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Recommendations For Testing, Managing, and Treating Hepatitis C - HCV TESTING and LINKAGE To CARE - 2015-06-29Документ12 страницRecommendations For Testing, Managing, and Treating Hepatitis C - HCV TESTING and LINKAGE To CARE - 2015-06-29malik003Оценок пока нет
- Visa Sopporting Documents Attach List: Dr. Zaheer Ahmed, MBBSДокумент1 страницаVisa Sopporting Documents Attach List: Dr. Zaheer Ahmed, MBBSmalik003Оценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- SummariesДокумент140 страницSummariesmalik003Оценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- April 24: Zein Mahgoub PACES Simplified Zein MahgoubДокумент4 страницыApril 24: Zein Mahgoub PACES Simplified Zein Mahgoubmalik003Оценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Bleeding Disorder ApproachДокумент9 страницBleeding Disorder Approachmalik003Оценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Dha Exam..Muhammad IbrahimДокумент11 страницDha Exam..Muhammad Ibrahimmalik003100% (4)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Unilateral Enlarged Kidney PDFДокумент2 страницыUnilateral Enlarged Kidney PDFmalik003Оценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Cranial Nerve AssessmentДокумент42 страницыCranial Nerve Assessmentmalik003100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Recommendations For Testing, Managing, and Treating Hepatitis C - MANAGEMENT of ACUTE HCV INFECTION - 2015-06-29Документ8 страницRecommendations For Testing, Managing, and Treating Hepatitis C - MANAGEMENT of ACUTE HCV INFECTION - 2015-06-29malik003Оценок пока нет
- CVS PDFДокумент102 страницыCVS PDFmalik003Оценок пока нет
- 6868841Документ35 страниц6868841malik003Оценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Prevention of Venous Thromboembolism in Nonsurgical PatientsДокумент23 страницыPrevention of Venous Thromboembolism in Nonsurgical Patientsmalik003Оценок пока нет
- GR 080013Документ3 страницыGR 080013malik003Оценок пока нет
- Urgent Required Female Staff NursesДокумент1 страницаUrgent Required Female Staff Nursesmalik003Оценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- New Doc 44 - 1Документ1 страницаNew Doc 44 - 1malik003Оценок пока нет
- 5446.full 2Документ12 страниц5446.full 2malik003Оценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
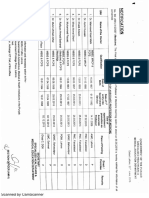
- Assoc Prof MedДокумент1 страницаAssoc Prof Medmalik003Оценок пока нет
- 1000 Prometric MCQ Solved 2Документ351 страница1000 Prometric MCQ Solved 2chronos653490% (106)
- Associate MedДокумент2 страницыAssociate Medmalik003Оценок пока нет
- Associate Med PDFДокумент2 страницыAssociate Med PDFmalik003Оценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Process Recording LGДокумент8 страницProcess Recording LGSolsona Natl HS MaanantengОценок пока нет
- End Semester SyllabusДокумент6 страницEnd Semester SyllabusHazel RoyОценок пока нет
- Resume 2021Документ3 страницыResume 2021api-558180395Оценок пока нет
- Food and Beverages Cantianing Aloe VeraДокумент16 страницFood and Beverages Cantianing Aloe VerairfanaliОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Karly Perkins - Annotated BibliographyДокумент7 страницKarly Perkins - Annotated Bibliographyapi-282594122Оценок пока нет
- Week 2 Lesson 1 2 - Quantitative Research, Characteristics and ImportanceДокумент13 страницWeek 2 Lesson 1 2 - Quantitative Research, Characteristics and ImportanceMicaela CastilloОценок пока нет
- Midterm Ca1 (1) CHNДокумент7 страницMidterm Ca1 (1) CHNRheeanne Mae AmilasanОценок пока нет
- Documentary On Emotional IntelligenceДокумент28 страницDocumentary On Emotional IntelligencelyvabreraОценок пока нет
- Anton GroupДокумент12 страницAnton Groupjerick veranoОценок пока нет
- Research Title ProposalДокумент7 страницResearch Title ProposalHazel GumaponОценок пока нет
- Posluns, K. & Lynn Gall, T. (2019) - Dear Mental Health Practitioners, Take Care of Yourselves, A Literature Review On Self-Care.Документ20 страницPosluns, K. & Lynn Gall, T. (2019) - Dear Mental Health Practitioners, Take Care of Yourselves, A Literature Review On Self-Care.MARIO APPELIUS SANHUEZAОценок пока нет
- W1 - Module-001 - Defining Popular CultureДокумент4 страницыW1 - Module-001 - Defining Popular CultureDanica VetuzОценок пока нет
- Alternative Ways in Assessing Learning 2Документ15 страницAlternative Ways in Assessing Learning 2Marra EscaranОценок пока нет
- Lit 3Документ9 страницLit 3Chezka BristolОценок пока нет
- The Radionic Association LibraryДокумент27 страницThe Radionic Association LibrarycristikissОценок пока нет
- Cooper Pharmaceuticals, IncДокумент4 страницыCooper Pharmaceuticals, IncParvezshAhamedОценок пока нет
- (Edited) N31-G6-SOP-and-Conceptual-FrameworkДокумент5 страниц(Edited) N31-G6-SOP-and-Conceptual-Frameworkst michael machine shopОценок пока нет
- Bsed-Engl 2 Iñego, Jhyrine EDFTC 105 Suganob, AbbygayleДокумент2 страницыBsed-Engl 2 Iñego, Jhyrine EDFTC 105 Suganob, AbbygayleAbbygayle SuganobОценок пока нет
- American Indian Family PatternsДокумент11 страницAmerican Indian Family PatternsRobin KeatingОценок пока нет
- Wolfe Nature vs. Nurture ProjectДокумент3 страницыWolfe Nature vs. Nurture ProjectCarla WolfeОценок пока нет
- MODULE#1 - LESSON#2 Ability and DisabilityДокумент8 страницMODULE#1 - LESSON#2 Ability and DisabilityClarissa L. NoelОценок пока нет
- Emotional Intelligence in The Workplace HSC 2015Документ44 страницыEmotional Intelligence in The Workplace HSC 2015Mohammad Mesbaul HaqueОценок пока нет
- Dr. Ghali Resignation Letter To LSUДокумент2 страницыDr. Ghali Resignation Letter To LSURachael ThomasОценок пока нет
- Margie's Travel: Let Margie Plan Your Next Winter Vacation!Документ2 страницыMargie's Travel: Let Margie Plan Your Next Winter Vacation!Alex TorresОценок пока нет
- Conquering Self Sabotaging Views Part A COD WorksheetДокумент2 страницыConquering Self Sabotaging Views Part A COD WorksheetKris PitmanОценок пока нет
- Attitude InventoryДокумент3 страницыAttitude InventoryAlexander SaladinОценок пока нет
- Examining Ways That A Mindfulness-Based Intervention Reduces Stress in Public School TeachersДокумент16 страницExamining Ways That A Mindfulness-Based Intervention Reduces Stress in Public School TeachersAlícia NascimentoОценок пока нет
- Abnormal Psychology CIA 1Документ4 страницыAbnormal Psychology CIA 1JoshuaОценок пока нет
- DEFENSEДокумент7 страницDEFENSELacanaria, Sandra G.Оценок пока нет
- O'Reilly-1997-Journal of Applied Behavior AnalysisДокумент3 страницыO'Reilly-1997-Journal of Applied Behavior AnalysisTimiОценок пока нет
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryОт EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryРейтинг: 4.5 из 5 звезд4.5/5 (157)
- Redefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackОт EverandRedefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackРейтинг: 4.5 из 5 звезд4.5/5 (153)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeОт EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeРейтинг: 4.5 из 5 звезд4.5/5 (140)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDОт EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDРейтинг: 4.5 из 5 звезд4.5/5 (167)