Вам также может понравиться
- Aaaaaa KKДокумент1 страницаAaaaaa KKArinta Purwi SuhartiОценок пока нет
- NPH 12325Документ17 страницNPH 12325Arinta Purwi SuhartiОценок пока нет
- (2004, Bailey DKK) Prediction of Anti-Plasmodial Activity of A Annua - Application of 1H NMR Spectroscopy and ChemometricsДокумент10 страниц(2004, Bailey DKK) Prediction of Anti-Plasmodial Activity of A Annua - Application of 1H NMR Spectroscopy and ChemometricsArinta Purwi SuhartiОценок пока нет
- (2012 Ye & Bhatia) REVIEW - Metabolic Engineering For The Production of Clinically Important Molecules - Omega-3 Fatty Acids, Artemisinin, and TaxolДокумент14 страниц(2012 Ye & Bhatia) REVIEW - Metabolic Engineering For The Production of Clinically Important Molecules - Omega-3 Fatty Acids, Artemisinin, and TaxolArinta Purwi SuhartiОценок пока нет
- IJAMSCR 14 205 SreenagavalliДокумент3 страницыIJAMSCR 14 205 SreenagavalliArinta Purwi SuhartiОценок пока нет
- (2009, Anthony DKK) Optimization of The Mevalonate-Based Isoprenoid Biosynthetic in E Coli For Production Amorpha-4,11-DieneДокумент7 страниц(2009, Anthony DKK) Optimization of The Mevalonate-Based Isoprenoid Biosynthetic in E Coli For Production Amorpha-4,11-DieneArinta Purwi SuhartiОценок пока нет
- Molecules 15 00040Документ18 страницMolecules 15 00040Arinta Purwi SuhartiОценок пока нет
- (2002 Wentzinger DKK) Inhibition of Squalene Synthase and Squalene Epoxidase in Tobacco Cells Triggers An Up-Regulation of 3-Hydroxy-3-Methylglutaryl Coenzyme A Reductase PDFДокумент13 страниц(2002 Wentzinger DKK) Inhibition of Squalene Synthase and Squalene Epoxidase in Tobacco Cells Triggers An Up-Regulation of 3-Hydroxy-3-Methylglutaryl Coenzyme A Reductase PDFArinta Purwi SuhartiОценок пока нет
- 03 AДокумент10 страниц03 AArinta Purwi SuhartiОценок пока нет
- (2013 Pu DKK) Expression and Localization of Amorpha-4,11-Diene Synthase in Artemisia Annua L.Документ6 страниц(2013 Pu DKK) Expression and Localization of Amorpha-4,11-Diene Synthase in Artemisia Annua L.Arinta Purwi SuhartiОценок пока нет
- Inhibitory Effects of Artemisinin On Voltage-Gated Ion Channels in Intact Nodose Ganglion Neurones of Adult RatsДокумент8 страницInhibitory Effects of Artemisinin On Voltage-Gated Ion Channels in Intact Nodose Ganglion Neurones of Adult RatsArinta Purwi SuhartiОценок пока нет
- Journal Pone 0068231Документ8 страницJournal Pone 0068231bhatubimОценок пока нет
- Antimicrobial Activity of Crude Extracts 2Документ6 страницAntimicrobial Activity of Crude Extracts 2Arinta Purwi SuhartiОценок пока нет
- Ni Hms 135180Документ19 страницNi Hms 135180Arinta Purwi SuhartiОценок пока нет
- Medicinal PlantsДокумент151 страницаMedicinal Plantsallanquartermaine0% (1)
- Finding Out About Cystic Fibrosis - A Guide For Parents: Factsheet - March 2013Документ22 страницыFinding Out About Cystic Fibrosis - A Guide For Parents: Factsheet - March 2013Arinta Purwi SuhartiОценок пока нет
- Antibiotic Treatment For Cystic FibrosisДокумент102 страницыAntibiotic Treatment For Cystic Fibrosischar1356Оценок пока нет
- Ni Hms 135180Документ19 страницNi Hms 135180Arinta Purwi SuhartiОценок пока нет
- KhawajaДокумент4 страницыKhawajaArinta Purwi SuhartiОценок пока нет
- FS Physio Babies and Toddlers Mar 13Документ7 страницFS Physio Babies and Toddlers Mar 13Arinta Purwi SuhartiОценок пока нет
- Antimicrobial Activity of Crude Extracts 2Документ6 страницAntimicrobial Activity of Crude Extracts 2Arinta Purwi SuhartiОценок пока нет
- MeleДокумент4 страницыMeleArinta Purwi SuhartiОценок пока нет
- Medicinal PlantsДокумент151 страницаMedicinal Plantsallanquartermaine0% (1)
- 5 Ajps 3 1 2013Документ4 страницы5 Ajps 3 1 2013Arinta Purwi SuhartiОценок пока нет
- HarrДокумент11 страницHarrArinta Purwi SuhartiОценок пока нет
- The Pathogenesis and Pathophysiology of Type 1 and PDFДокумент12 страницThe Pathogenesis and Pathophysiology of Type 1 and PDFasmawatiОценок пока нет
- Herbal Cosmetics for Beautiful Skin and HairДокумент9 страницHerbal Cosmetics for Beautiful Skin and HairBogdanОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Integrated disease management conceptsДокумент8 страницIntegrated disease management conceptsNidhi SinghОценок пока нет
- Ophthalmology - Diseases of CorneaДокумент18 страницOphthalmology - Diseases of CorneajbtcmdtjjvОценок пока нет
- MedChem10 Antiviral PDFДокумент85 страницMedChem10 Antiviral PDFMартин ДончевОценок пока нет
- RIZAL TECHNOLOGICAL UNIVERSITY NATIONAL SERVICE TRAINING PROGRAM MODULESДокумент9 страницRIZAL TECHNOLOGICAL UNIVERSITY NATIONAL SERVICE TRAINING PROGRAM MODULESJULIUS CAEZAR CHAVEZОценок пока нет
- Michael G. Glasspool FRCS, DO (Auth.) - Atlas of Ophthalmology-Springer Netherlands (1982) PDFДокумент117 страницMichael G. Glasspool FRCS, DO (Auth.) - Atlas of Ophthalmology-Springer Netherlands (1982) PDFInna BujorОценок пока нет
- Hepatitis B: DR Tanmay Vyas (DM Hepatology)Документ37 страницHepatitis B: DR Tanmay Vyas (DM Hepatology)Sreekanth VattikondaОценок пока нет
- Exually Tran Mitted Disease: Rean Jane EscabarteДокумент14 страницExually Tran Mitted Disease: Rean Jane EscabarteRan Jung EscabarteОценок пока нет
- Protein Calorie MalnutritionДокумент97 страницProtein Calorie Malnutritionnshaikh56Оценок пока нет
- SiriДокумент1 страницаSirisrinivasОценок пока нет
- India Today 18 March 2013Документ124 страницыIndia Today 18 March 2013Ravi SinghОценок пока нет
- Introduction and Neoplasia - PathologyДокумент20 страницIntroduction and Neoplasia - PathologyjmosserОценок пока нет
- ImpactionДокумент11 страницImpactionKhalid AgwaniОценок пока нет
- Gelect3 5Документ3 страницыGelect3 5Mhartin OrsalОценок пока нет
- Cancer ImmunologyДокумент12 страницCancer ImmunologyFreddy TorresОценок пока нет
- The Prevalence of Parasitic Protozoan Diseases in Iraq, 2016Документ5 страницThe Prevalence of Parasitic Protozoan Diseases in Iraq, 2016Jeremia AnkesaОценок пока нет
- Odessa National Medical University: Surgical InfectionsДокумент34 страницыOdessa National Medical University: Surgical InfectionsDrRajneesh ShastriОценок пока нет
- Herpes Simplex Type 1&2Документ15 страницHerpes Simplex Type 1&2ulfah febyОценок пока нет
- MycotoxinsДокумент20 страницMycotoxinsibraheem aboyadak100% (1)
- Expanded Program On Immunization Philippines)Документ8 страницExpanded Program On Immunization Philippines)Mark AcuzarОценок пока нет
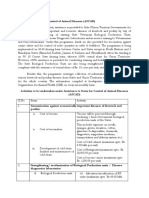
- Assistance To States For Control of Animal Diseases (ASCADДокумент6 страницAssistance To States For Control of Animal Diseases (ASCADMonal DaptardarОценок пока нет
- People at Virology: Dmitri Iosifovich Ivanovsky - Founders of VirologyДокумент2 страницыPeople at Virology: Dmitri Iosifovich Ivanovsky - Founders of VirologyFae BladeОценок пока нет
- NematodesДокумент4 страницыNematodesPrincess Shaina CanapeОценок пока нет
- Tuberculosis Lab ReportДокумент4 страницыTuberculosis Lab ReportJullian Clare CreusОценок пока нет
- Hot Topics in Internal MedicineДокумент9 страницHot Topics in Internal Medicinekhangsiean89Оценок пока нет
- Chikungunya - DINKES - RS UNAIR 22 November 2017Документ24 страницыChikungunya - DINKES - RS UNAIR 22 November 2017Mojo PuskesmasОценок пока нет
- Sanitary Engineering2 (Repaired)Документ95 страницSanitary Engineering2 (Repaired)ronnel mauzar100% (2)
- Litchi Heart Disease and It's ControlДокумент23 страницыLitchi Heart Disease and It's Controlpracholi lamp100% (1)
- Kumar Indoor Air Quality Study Summary - Proffer SweepsДокумент1 страницаKumar Indoor Air Quality Study Summary - Proffer SweepsAnonymous Pb39klJОценок пока нет
- Feline Dermatophytosis Treatment RecommendationsДокумент21 страницаFeline Dermatophytosis Treatment RecommendationsFrancisca Thenée SerranoОценок пока нет
- Causes of Sterile Pyuria Infection RelatedДокумент2 страницыCauses of Sterile Pyuria Infection RelatedSarah AhmedОценок пока нет