Вам также может понравиться
- Tactile Defensiveness PDFДокумент7 страницTactile Defensiveness PDFCristi BacuОценок пока нет
- An Integrated Approach - in Every SenseДокумент4 страницыAn Integrated Approach - in Every SenseSpeech & Language Therapy in PracticeОценок пока нет
- Sensory Diet DocumentsДокумент7 страницSensory Diet Documentspratibhaumrariya100% (1)
- Binocular Saccadic Dysfunction - a Precursor to Dyslexia?: N/AОт EverandBinocular Saccadic Dysfunction - a Precursor to Dyslexia?: N/AОценок пока нет
- Ot Guidelines Child SpecificДокумент34 страницыOt Guidelines Child Specific健康生活園Healthy Life Garden100% (1)
- How To Create A Successful, No-Stress Sensory Diet For Kids WorkbookДокумент4 страницыHow To Create A Successful, No-Stress Sensory Diet For Kids WorkbookAdriana NegrescuОценок пока нет
- Rheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementОт EverandRheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementLynne GoodacreОценок пока нет
- Clinical Observations of SIДокумент2 страницыClinical Observations of SIIsti Nisa100% (1)
- Occupational Therapy and Life Course Development: A Work Book for Professional PracticeОт EverandOccupational Therapy and Life Course Development: A Work Book for Professional PracticeОценок пока нет
- SI Theory and PracticeДокумент57 страницSI Theory and PracticeMaria Laura Soria100% (1)
- Marcus Evaluation - StruthersДокумент8 страницMarcus Evaluation - Struthersapi-355500890Оценок пока нет
- Milestone Chart For BabiesДокумент8 страницMilestone Chart For BabiesKaypee BorresОценок пока нет
- Sensory History QuestionnaireДокумент6 страницSensory History Questionnaireİpek OMUR100% (1)
- Space Management: 0 To 6 Months 6 To 12 Months 12 To 18 MonthsДокумент4 страницыSpace Management: 0 To 6 Months 6 To 12 Months 12 To 18 MonthsDaNelle McPhaddenОценок пока нет
- New Early Learning Progress Profile Documentation FormДокумент20 страницNew Early Learning Progress Profile Documentation Formapi-213387477Оценок пока нет
- Otor & Visual Motor AssessДокумент4 страницыOtor & Visual Motor AssessBea FloresОценок пока нет
- The Effect of A Two-Week Sensory Diet On Fussy Infants With Regulatory SensДокумент8 страницThe Effect of A Two-Week Sensory Diet On Fussy Infants With Regulatory Sensapi-238703581Оценок пока нет
- Ota Watertown Si Clinical Assessment WorksheetДокумент4 страницыOta Watertown Si Clinical Assessment WorksheetPaulinaОценок пока нет
- Ot Goals NuevoДокумент157 страницOt Goals NuevoElbania PerezОценок пока нет
- PT GoalsДокумент13 страницPT Goalsnaomi harowОценок пока нет
- Tummy Time Tip SheetДокумент3 страницыTummy Time Tip SheetEndahRatnaningrumОценок пока нет
- CO-OP PediatriaДокумент17 страницCO-OP PediatriaCarol Alvarado100% (2)
- Using The Infant/Toddler Sensory Profile in Early Intervention ServicesДокумент65 страницUsing The Infant/Toddler Sensory Profile in Early Intervention Servicesfitomena50% (2)
- Essential Mechanisms in Neurological Pediatric RehabilitationОт EverandEssential Mechanisms in Neurological Pediatric RehabilitationОценок пока нет
- CLASI Intervention Course NotesДокумент241 страницаCLASI Intervention Course Notessaskia.bouwer100% (1)
- Sensory Integration Inventory ItemiДокумент4 страницыSensory Integration Inventory Itemidragomir_emilia92Оценок пока нет
- Occupational Therapy Ia Sample ReportsДокумент11 страницOccupational Therapy Ia Sample Reportssneha duttaОценок пока нет
- Chapter 8Документ30 страницChapter 8Karla CarazoОценок пока нет
- A Review of Pediatric Assessment Tools For Sensory Integration AOTAДокумент3 страницыA Review of Pediatric Assessment Tools For Sensory Integration AOTAhelenzhang888Оценок пока нет
- Pediatric Evaluation ReportДокумент3 страницыPediatric Evaluation Reportapi-469965619Оценок пока нет
- OT Practice August 6 IssueДокумент19 страницOT Practice August 6 IssueThe American Occupational Therapy AssociationОценок пока нет
- Making Sense Out of Sensory Processing Disorder: Kay Kopp, OTR/L Tanyia Schier, MS, OTR/LДокумент61 страницаMaking Sense Out of Sensory Processing Disorder: Kay Kopp, OTR/L Tanyia Schier, MS, OTR/LKriti Shukla100% (1)
- Sensory Integration and Praxis Patterns in Children With AutismДокумент9 страницSensory Integration and Praxis Patterns in Children With AutismadriricaldeОценок пока нет
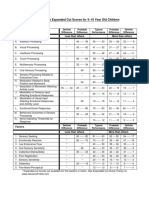
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenДокумент1 страницаSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliОценок пока нет
- Sensorimotor History Questionnaire For Parents of PreschoolДокумент77 страницSensorimotor History Questionnaire For Parents of Preschoolscribdmuthu100% (2)
- Azzam Scale in Practical Guide of Occupational TherapyОт EverandAzzam Scale in Practical Guide of Occupational TherapyОценок пока нет
- Double Time Docs Sample Evaluation OT SchoolДокумент10 страницDouble Time Docs Sample Evaluation OT SchoolAlyssa Balverde100% (1)
- AOTA Statement On Role of OT in NICUДокумент9 страницAOTA Statement On Role of OT in NICUMapi RuizОценок пока нет
- Sensory DietДокумент4 страницыSensory Dietapi-571361183Оценок пока нет
- Sensory Profile PowerpointДокумент21 страницаSensory Profile PowerpointFedora Margarita Santander CeronОценок пока нет
- Embedding Evidence-Based Practice in Speech and Language Therapy: International ExamplesОт EverandEmbedding Evidence-Based Practice in Speech and Language Therapy: International ExamplesHazel RoddamРейтинг: 5 из 5 звезд5/5 (1)
- Play Behavior and Occupational TherapyДокумент9 страницPlay Behavior and Occupational TherapyaaaОценок пока нет
- Sensory Diet Sample FormatДокумент1 страницаSensory Diet Sample FormatBernard CarpioОценок пока нет
- Occupation Analysis in PracticeОт EverandOccupation Analysis in PracticeLynette MackenzieОценок пока нет
- Activity Monitoring WorksheetДокумент2 страницыActivity Monitoring WorksheetRoberto SzenczukОценок пока нет
- Occupational Therapy Evaluation Report and Initial Intervention PlanДокумент12 страницOccupational Therapy Evaluation Report and Initial Intervention Planapi-488383880100% (1)
- Evaluation ReportДокумент3 страницыEvaluation Reportapi-547360536Оценок пока нет
- Clients Goals To Address in SessionДокумент8 страницClients Goals To Address in Sessionapi-436429414Оценок пока нет
- Helping Hands-Website InformationДокумент17 страницHelping Hands-Website InformationDiana Moore Díaz100% (1)
- Sensory Processing BrochureДокумент3 страницыSensory Processing Brochureapi-383884645Оценок пока нет
- Senior Occupational Therapist: Passbooks Study GuideОт EverandSenior Occupational Therapist: Passbooks Study GuideОценок пока нет
- Pediatric Wheelchair Toolkit FINALДокумент6 страницPediatric Wheelchair Toolkit FINALIndiana Family to FamilyОценок пока нет
- Working With Children With Atypical Tone 07Документ37 страницWorking With Children With Atypical Tone 07Martha FrankОценок пока нет
- Chapter 16: Application of Motor Control and Motor LearningДокумент8 страницChapter 16: Application of Motor Control and Motor LearningJireh Chambers100% (1)
- Student Treatment Session Soap 8Документ9 страницStudent Treatment Session Soap 8api-340625860100% (1)
- HelpДокумент20 страницHelpsurender_singh_430% (1)
- Sensory AssesmentДокумент19 страницSensory AssesmentBurçin KaynakОценок пока нет
- 13clinical ReasoningДокумент6 страниц13clinical ReasoningAnup PednekarОценок пока нет
- Visual SkillsДокумент8 страницVisual SkillsAnup PednekarОценок пока нет
- Pressure, Temperature, Pain, and Movement of The Hairs On The SkinДокумент18 страницPressure, Temperature, Pain, and Movement of The Hairs On The SkinAnup PednekarОценок пока нет
- SPDДокумент24 страницыSPDAnup PednekarОценок пока нет
- Graphomotor SkillsДокумент5 страницGraphomotor SkillsMiss MarijaОценок пока нет
- Theme: - Date: - Lesson Plan (Quick View)Документ1 страницаTheme: - Date: - Lesson Plan (Quick View)Anup PednekarОценок пока нет
- Ocular Motor ActivitiesДокумент1 страницаOcular Motor ActivitiesAnup PednekarОценок пока нет
- Mailloux May BensonДокумент6 страницMailloux May BensonAnup Pednekar100% (1)
- Choose A Career With MeaningДокумент2 страницыChoose A Career With MeaningAnup PednekarОценок пока нет
- GRH Freeport Site TravelДокумент3 страницыGRH Freeport Site TravelAnup PednekarОценок пока нет
- Sumber 3Документ6 страницSumber 3AlFi KamaliaОценок пока нет
- Lock Box Obligation PHIPAДокумент4 страницыLock Box Obligation PHIPAAnup PednekarОценок пока нет
- Npte CDДокумент1 страницаNpte CDAnup PednekarОценок пока нет
- Choose A Career With MeaningДокумент2 страницыChoose A Career With MeaningAnup PednekarОценок пока нет
- Congestive Heart FailureДокумент37 страницCongestive Heart FailurePierre Aseron ManuelОценок пока нет
- Musculoskeletal Program of Care (MSK Poc) : Patient-Specific Functional Scale (PSFS)Документ1 страницаMusculoskeletal Program of Care (MSK Poc) : Patient-Specific Functional Scale (PSFS)Anup PednekarОценок пока нет
- Objective #4: Test Your Knowledge - ANSWERSДокумент1 страницаObjective #4: Test Your Knowledge - ANSWERSAnup PednekarОценок пока нет
- Breast Feeding and LctationДокумент9 страницBreast Feeding and LctationAnup PednekarОценок пока нет
- Suspension TherapyДокумент43 страницыSuspension TherapyAnup Pednekar0% (1)
- Sneh RERC Advanced Sensory Integration Workshop January 2014Документ4 страницыSneh RERC Advanced Sensory Integration Workshop January 2014Anup PednekarОценок пока нет
- SupportWorkerPosting KWHabilitation Aug2014Документ1 страницаSupportWorkerPosting KWHabilitation Aug2014Anup PednekarОценок пока нет
- 300 Red Osier RD Anup PednekarДокумент1 страница300 Red Osier RD Anup PednekarAnup PednekarОценок пока нет
- Model Teaching: Teaching The NDT Enablement Classification of Health and DisabilityДокумент9 страницModel Teaching: Teaching The NDT Enablement Classification of Health and DisabilityAnup PednekarОценок пока нет
- Energy Expenditure in CPДокумент8 страницEnergy Expenditure in CPAnup PednekarОценок пока нет
- Thank You: This Powerpoint Document Contains The Images That You RequestedДокумент5 страницThank You: This Powerpoint Document Contains The Images That You RequestedAnup PednekarОценок пока нет
- Diane DaminoДокумент11 страницDiane DaminoAnup PednekarОценок пока нет
- Determinants of GaitДокумент35 страницDeterminants of GaitAnup Pednekar50% (2)
- Collins Robot Press ScienceNewsДокумент6 страницCollins Robot Press ScienceNewsAnup PednekarОценок пока нет
- Topic 2: Understanding The Arts: at The End of The Session, You Will Be Able ToДокумент5 страницTopic 2: Understanding The Arts: at The End of The Session, You Will Be Able ToAbigail Delos SantosОценок пока нет
- Personal Development: Module 1: Knowing and Understanding Oneself During Middle and Late AdolescenceДокумент6 страницPersonal Development: Module 1: Knowing and Understanding Oneself During Middle and Late AdolescenceJasmin MateoОценок пока нет
- Correction Assignment Consumer BehaviourДокумент4 страницыCorrection Assignment Consumer BehaviourHassen OmriОценок пока нет
- Neuro-Linguistic Programming For Dummies Cheat Sheet - For DummiesДокумент4 страницыNeuro-Linguistic Programming For Dummies Cheat Sheet - For DummiesNadia Lucía VazquezОценок пока нет
- Theories of LearningДокумент32 страницыTheories of LearningJoel Sempijja100% (1)
- 2 CognitionДокумент2 страницы2 Cognitionapi-110970813Оценок пока нет
- 21 Century of PsycolinguisticsДокумент423 страницы21 Century of Psycolinguisticsnovrique100% (5)
- IshiharaДокумент25 страницIshiharaHarika PutraОценок пока нет
- JoeVitale 3DayRuleДокумент56 страницJoeVitale 3DayRuleGilbert SimpsonОценок пока нет
- Tuhog ReflectionДокумент2 страницыTuhog ReflectionCATHERINE SIENNA ALTARОценок пока нет
- Whatis IntelligenceДокумент15 страницWhatis IntelligenceSahilPrabhakarОценок пока нет
- Responses 003Документ1 страницаResponses 003Aamir ShaikОценок пока нет
- Calasanz, Eduardo. Ateneo de Manila University. Mr. Renz Joelle C. Domingo - Holy Spirit Academy of MalolosДокумент32 страницыCalasanz, Eduardo. Ateneo de Manila University. Mr. Renz Joelle C. Domingo - Holy Spirit Academy of MalolosG03 Alfonso, Rochelle ElaineОценок пока нет
- Ausubel's Theory of Meaningful LearningДокумент4 страницыAusubel's Theory of Meaningful LearningRadhaSharma100% (4)
- ENTP User Guide and ManualДокумент8 страницENTP User Guide and ManualMerima VukotićОценок пока нет
- Colligan Cep800 PersonaltheoryoflearningДокумент9 страницColligan Cep800 Personaltheoryoflearningapi-310814251Оценок пока нет
- The Great Gatsby Imagery AssignmentДокумент3 страницыThe Great Gatsby Imagery AssignmentruchinidissanayakeОценок пока нет
- Chapter 10Документ5 страницChapter 10Lorie Jane UngabОценок пока нет
- Thirty Years and Counting: Finding Meaning in The N400 Component of The Event-Related Brain Potential (ERP)Документ32 страницыThirty Years and Counting: Finding Meaning in The N400 Component of The Event-Related Brain Potential (ERP)kickinghorse892Оценок пока нет
- Learning Module: Zamboanga Peninsula Polytechnic State UniversityДокумент44 страницыLearning Module: Zamboanga Peninsula Polytechnic State UniversityCharmelyn Jane GuevarraОценок пока нет
- Defining The Self: Personal and Developmental Perspectives On Self and IdentityДокумент19 страницDefining The Self: Personal and Developmental Perspectives On Self and IdentityCelina Jane MagpantayОценок пока нет
- NST IB-PBS4 Course Guide 2022-23 24.11.2022Документ32 страницыNST IB-PBS4 Course Guide 2022-23 24.11.2022Bright AlanОценок пока нет
- Group 3 - Core of SciencesДокумент10 страницGroup 3 - Core of Sciencesapi-557677480Оценок пока нет
- Testing ReadingДокумент19 страницTesting ReadingCharisse Karen RodreguezОценок пока нет
- Nasionalism: Character Education Orientation in Learning DevelopmentДокумент9 страницNasionalism: Character Education Orientation in Learning DevelopmentFriska Adelia SariОценок пока нет
- Module Ed 111 Professional EnhancementДокумент270 страницModule Ed 111 Professional EnhancementRomelene GalacinaoОценок пока нет
- Unit 4 Study GuideДокумент4 страницыUnit 4 Study GuideVanshika GuptaОценок пока нет
- Contemporary Learning Theories/Psychologists: Their Impact To EPP TeachingДокумент5 страницContemporary Learning Theories/Psychologists: Their Impact To EPP TeachingAlexis Kaye GullaОценок пока нет
- LESSON 5 Officiating StylesДокумент15 страницLESSON 5 Officiating Styleslilibeth palinoОценок пока нет
- Philosopher's Gallery Walk - Class: Jefferson DaoatinДокумент5 страницPhilosopher's Gallery Walk - Class: Jefferson DaoatinKelsey BarcelОценок пока нет