Вам также может понравиться
- B - Respiratory PhysiologyДокумент73 страницыB - Respiratory PhysiologyMohamad Zekry ZuhairyОценок пока нет
- D - Renal PhysiologyДокумент26 страницD - Renal PhysiologyMohamad Zekry ZuhairyОценок пока нет
- C - Cardiovascular PhysiologyДокумент61 страницаC - Cardiovascular PhysiologyMohamad Zekry ZuhairyОценок пока нет
- A - Cellular PhysiologyДокумент12 страницA - Cellular PhysiologyMohamad Zekry ZuhairyОценок пока нет
- Rapid Sequence InductionДокумент8 страницRapid Sequence InductionAngela Mitchelle NyanganОценок пока нет
- Body Fluids & ElectrolytesДокумент26 страницBody Fluids & ElectrolytesMohamad Zekry Zuhairy100% (1)
- Khairyst O Khairy Hafizy Turn 10 Happy BirthdayДокумент3 страницыKhairyst O Khairy Hafizy Turn 10 Happy BirthdayMohamad Zekry ZuhairyОценок пока нет
- Rapid Sequence InductionДокумент8 страницRapid Sequence InductionAngela Mitchelle NyanganОценок пока нет
- Rapid Sequence InductionДокумент8 страницRapid Sequence InductionAngela Mitchelle NyanganОценок пока нет
- Rapid Sequence InductionДокумент8 страницRapid Sequence InductionAngela Mitchelle NyanganОценок пока нет
- Suicide Risk Assessment and ManagementДокумент6 страницSuicide Risk Assessment and ManagementMohamad Zekry ZuhairyОценок пока нет
- Table15 TypesofHazardДокумент1 страницаTable15 TypesofHazardJackie HwangОценок пока нет
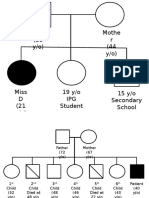
- Geneological ChartДокумент2 страницыGeneological ChartMohamad Zekry ZuhairyОценок пока нет
- Endometrial CAДокумент74 страницыEndometrial CAMohamad Zekry ZuhairyОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Pestle Analysis of Cdo-Foodspear Inc.: Science City of Munoz, Nueva EcijaДокумент6 страницPestle Analysis of Cdo-Foodspear Inc.: Science City of Munoz, Nueva EcijaPrincess NietoОценок пока нет
- Definition of GriefДокумент16 страницDefinition of GriefNaveen Eldose100% (1)
- AIA 6600 - Module 3 - Milestone 1 - Artificial Intelligence Product Portfolio in The Healthcare IndustryДокумент6 страницAIA 6600 - Module 3 - Milestone 1 - Artificial Intelligence Product Portfolio in The Healthcare Industryedna.ejimakorОценок пока нет
- Clinical Practice Guidelines and ProtocolsДокумент4 страницыClinical Practice Guidelines and ProtocolsMahmoud NaggarОценок пока нет
- Unit 4 Maternal ConceptsДокумент8 страницUnit 4 Maternal ConceptsEunice TrinidadОценок пока нет
- I Hi Trigger Tool For Measuring Adverse Drug EventsДокумент16 страницI Hi Trigger Tool For Measuring Adverse Drug EventsGaby ValenzuelaОценок пока нет
- CMS MLN Cognitive Assessment and Care Plan Services CPT Code 99483Документ4 страницыCMS MLN Cognitive Assessment and Care Plan Services CPT Code 99483Salomon GreenОценок пока нет
- Zahid RevisedДокумент7 страницZahid Revisedrokeya tamannaОценок пока нет
- Review Article: Common Periodontal Diseases of Children and AdolescentsДокумент8 страницReview Article: Common Periodontal Diseases of Children and AdolescentsGea Akalili SabrinaОценок пока нет
- Cumbria and Lancs KCN Algorithm PDFДокумент18 страницCumbria and Lancs KCN Algorithm PDFratih83Оценок пока нет
- Nutrition. Write The Information in Black, Fill in The Blanks and Answer All of The Questions in RedДокумент3 страницыNutrition. Write The Information in Black, Fill in The Blanks and Answer All of The Questions in Rednoddy60Оценок пока нет
- Bpacnz Antibiotics GuideДокумент40 страницBpacnz Antibiotics GuideBulborea MihaelaОценок пока нет
- Law and MedicineДокумент2 страницыLaw and MedicineCP Ispat Unit IIОценок пока нет
- Adult Nutrition Assessment Tutorial 2012Документ9 страницAdult Nutrition Assessment Tutorial 2012Dariana floresОценок пока нет
- A Clinical Study of Siddha Herbal Preparation - M V Kashayam For The Treatment, Control, and Management of Covid-19Документ4 страницыA Clinical Study of Siddha Herbal Preparation - M V Kashayam For The Treatment, Control, and Management of Covid-19Mor ThyОценок пока нет
- 1st Grading Exam MAPEHДокумент4 страницы1st Grading Exam MAPEHSherlita Vargas Mainit DurogОценок пока нет
- Course - Fundamentals of Traditional Chinese Medicine - Center For True HealingДокумент49 страницCourse - Fundamentals of Traditional Chinese Medicine - Center For True HealingAry Nogueira100% (1)
- Non-Hemolytic Transfusion ReactionДокумент32 страницыNon-Hemolytic Transfusion Reactiondreyngerous100% (4)
- Lost All HopeДокумент8 страницLost All HopeRhemiel Castañeda100% (1)
- Family PlanningДокумент15 страницFamily PlanningOkky isОценок пока нет
- Prepatellar Bursitis - Housemaid's KneeДокумент2 страницыPrepatellar Bursitis - Housemaid's KneeenadОценок пока нет
- The Pathophysiologic Basis of Nuclear MedicineДокумент21 страницаThe Pathophysiologic Basis of Nuclear MedicineShazia FatimaОценок пока нет
- Prognostic Indicators in Differentiated Thyroid Carcinoma: Diana S. Dean, MD, and Ian D. Hay, MB, PHD, FRCPДокумент11 страницPrognostic Indicators in Differentiated Thyroid Carcinoma: Diana S. Dean, MD, and Ian D. Hay, MB, PHD, FRCPRum Afida RasfaОценок пока нет
- Epidemiology, Pathology, Clinical Features, and Diagnosis of Meningioma - UpToDateДокумент22 страницыEpidemiology, Pathology, Clinical Features, and Diagnosis of Meningioma - UpToDatewilson kores100% (1)
- IELTS MASTER IELTS Listening Test 135Документ1 страницаIELTS MASTER IELTS Listening Test 135arina.pylypetsОценок пока нет
- Library - Uns.ac - Id Digilib - Uns.ac - Id: Daftar PustakaДокумент6 страницLibrary - Uns.ac - Id Digilib - Uns.ac - Id: Daftar PustakaJulistin haiОценок пока нет
- Typhoid FeverДокумент20 страницTyphoid FeverKylie GolindangОценок пока нет
- Date Performed: Final Grade: Clinical Instructor: Administering Eye Medication DefinitionДокумент3 страницыDate Performed: Final Grade: Clinical Instructor: Administering Eye Medication Definitionhjl padillaОценок пока нет
- Fibromyalgia: Invisible Pain (Body Image and Depression)Документ8 страницFibromyalgia: Invisible Pain (Body Image and Depression)4gen_3Оценок пока нет
- TOYOTA SR 09 - EngagingEmployees PDFДокумент11 страницTOYOTA SR 09 - EngagingEmployees PDFurooj salmanОценок пока нет