Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Physical Assessment For Stroke PatientДокумент4 страницыPhysical Assessment For Stroke Patientdana75% (4)
- Nephrocalcinosis - UpToDateДокумент19 страницNephrocalcinosis - UpToDateRICO NOVYANTOОценок пока нет
- Deep Venous Thrombosis After Radical Pelvic Surgery: March 2012Документ13 страницDeep Venous Thrombosis After Radical Pelvic Surgery: March 2012Fasihul LizanОценок пока нет
- MalrotasiДокумент6 страницMalrotasiFasihul LizanОценок пока нет
- Amputasi Bellow KneeДокумент29 страницAmputasi Bellow KneeFasihul LizanОценок пока нет
- Total Thyroidectomy The Evolution ofДокумент8 страницTotal Thyroidectomy The Evolution ofFasihul Lizan100% (1)
- Endocrinology Endocrine System Review SheetДокумент6 страницEndocrinology Endocrine System Review SheetRazvan SerbanОценок пока нет
- Lecture On The Histology of Cerebrum and Meninges by Dr. RoomiДокумент20 страницLecture On The Histology of Cerebrum and Meninges by Dr. RoomiMudassar Roomi100% (1)
- Massaging Auricular PointsДокумент2 страницыMassaging Auricular PointsCarissa Nichols100% (5)
- Pituitary Gland Anatomy: Embryologic DevelopmentДокумент9 страницPituitary Gland Anatomy: Embryologic DevelopmentRafaelPetitОценок пока нет
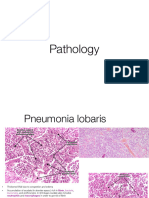
- Pathology Seminar Review (Semester 1)Документ26 страницPathology Seminar Review (Semester 1)Lin AdutОценок пока нет
- Detailed LP Science DemoДокумент12 страницDetailed LP Science DemoMau AcusaОценок пока нет
- Cardiovascular AssessmentДокумент13 страницCardiovascular AssessmentKathryn Bianca AcanceОценок пока нет
- The Reproductive System1Документ19 страницThe Reproductive System1Elijah Mae CubaОценок пока нет
- Kuliah 3. Biosintesis Dan Mekanisme Kerja Hormon Reproduksi PriaДокумент38 страницKuliah 3. Biosintesis Dan Mekanisme Kerja Hormon Reproduksi PriaYulia Fatma NstОценок пока нет
- Final Hydrocephalus Care PlanДокумент11 страницFinal Hydrocephalus Care PlanSAYMABANUОценок пока нет
- Nerve Muscle PhysioДокумент30 страницNerve Muscle Physiopatel_hanisha06Оценок пока нет
- History Essay ExamplesДокумент6 страницHistory Essay Examplesb72d994zОценок пока нет
- Subjective: Goals: - : Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationДокумент18 страницSubjective: Goals: - : Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationJennalyn Padua SevillaОценок пока нет
- (Mebooksfree Net) Chr&kid&dis&dia&tre&yan&he&1st PDFДокумент250 страниц(Mebooksfree Net) Chr&kid&dis&dia&tre&yan&he&1st PDFmainoОценок пока нет
- Angiology NoteДокумент13 страницAngiology NoteSantosh Bhandari100% (2)
- Cute and Hronic: Renal FailureДокумент31 страницаCute and Hronic: Renal FailureEhab S. AlHarbiОценок пока нет
- AbnormalitiesДокумент17 страницAbnormalitiesDitta Nur apriantyОценок пока нет
- CH 03Документ26 страницCH 03asmaa aldraiwieshОценок пока нет
- Adrenal InsufficiencyДокумент15 страницAdrenal InsufficiencyJuvial DavidОценок пока нет
- Lect. 33 Lymphoid System 2Документ36 страницLect. 33 Lymphoid System 2Christine eleyi - OkparaОценок пока нет
- Lab Report Bio560Документ31 страницаLab Report Bio560Alis SyamimiОценок пока нет
- BasicScienceYear10textbook PDFДокумент133 страницыBasicScienceYear10textbook PDFDove PaeaОценок пока нет
- Abdominal OrgansДокумент132 страницыAbdominal OrgansSheryl Layne LaoОценок пока нет
- Spinal Cord AnatomyДокумент20 страницSpinal Cord AnatomyrooparawatОценок пока нет
- Cardiovascular System - Heart IntroДокумент6 страницCardiovascular System - Heart IntroKate Angeline TanОценок пока нет
- Far Eastern University Institue of Arts and Science Department of Medical Technology Histology 2 SEMESTER AY 2020-2021Документ1 страницаFar Eastern University Institue of Arts and Science Department of Medical Technology Histology 2 SEMESTER AY 2020-2021Kaye RiofloridoОценок пока нет
- Anatomy and Physiology-NotesДокумент6 страницAnatomy and Physiology-NotesAkirah Jewelle JaenОценок пока нет
- Dho Health Science Updated 8th Edition Simmers Test BankДокумент9 страницDho Health Science Updated 8th Edition Simmers Test Bankjosephrodriguez04121993gbm100% (27)