Вам также может понравиться
- Water Music: Minuet and AirДокумент3 страницыWater Music: Minuet and AirRodrigo PessoaОценок пока нет
- Herrera School Buses, Inc.-Vendor#40464: Review, Sign, With PO# or Payment and Return at Least 1 Week Prior To TripДокумент2 страницыHerrera School Buses, Inc.-Vendor#40464: Review, Sign, With PO# or Payment and Return at Least 1 Week Prior To TripRodrigo PessoaОценок пока нет
- Ent ErДокумент1 страницаEnt ErRodrigo PessoaОценок пока нет
- 3 PDFДокумент1 страница3 PDFRodrigo PessoaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- B2 UNIT 4 Test StandardДокумент6 страницB2 UNIT 4 Test StandardВладимир РанцовОценок пока нет
- Global Perspectives Reflective PaperДокумент3 страницыGlobal Perspectives Reflective PaperMoaiz AttiqОценок пока нет
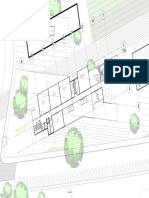
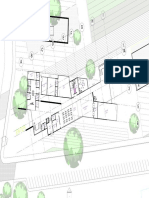
- Urban Square Design: Landscape Design Studio III LAR 803Документ44 страницыUrban Square Design: Landscape Design Studio III LAR 803Peter DokpesiОценок пока нет
- GnatusДокумент36 страницGnatusNacer Mezghiche100% (1)
- 850 Elective English QPДокумент3 страницы850 Elective English QPRudra SahaОценок пока нет
- Student Exam FormДокумент4 страницыStudent Exam FormRaj Kumar TeotiaОценок пока нет
- Literature Review Electrical EngineeringДокумент6 страницLiterature Review Electrical Engineeringtkpmzasif100% (1)
- Part D - Disclosure and TransparencyДокумент21 страницаPart D - Disclosure and TransparencyMuhammadYudithEddwinaОценок пока нет
- Individual Ability in SoftwareДокумент9 страницIndividual Ability in Softwaredhana0809100% (4)
- Distortion of The Ecclesiological Views of Metropolitan Chrysostomos of PhlorinaДокумент11 страницDistortion of The Ecclesiological Views of Metropolitan Chrysostomos of PhlorinaHibernoSlavОценок пока нет
- Students List - All SectionsДокумент8 страницStudents List - All SectionsChristian RiveraОценок пока нет
- Govt Considers Putting ShahbazДокумент27 страницGovt Considers Putting ShahbazWanderer123Оценок пока нет
- Exercise No. 2 (DCC First and Second Summary)Документ3 страницыExercise No. 2 (DCC First and Second Summary)Lalin-Mema LRОценок пока нет
- Apy1 Kinematics Review - 2015 - KeyДокумент13 страницApy1 Kinematics Review - 2015 - KeyemadОценок пока нет
- Impact of Empathy in The Patient-DoctorДокумент11 страницImpact of Empathy in The Patient-DoctorFauzan AnugrahОценок пока нет
- QAS M001 SLPS Quality Assurance ManualДокумент49 страницQAS M001 SLPS Quality Assurance ManualMHDОценок пока нет
- CCSI - HDPE - Subduct 50-4240-33 32-27 32-28 - Rev.0 - TelkomДокумент1 страницаCCSI - HDPE - Subduct 50-4240-33 32-27 32-28 - Rev.0 - TelkomAlvan umaraОценок пока нет
- PRP RationaleДокумент12 страницPRP Rationalemarquezjayson548Оценок пока нет
- CREW Whitaker Recusal Letter DOJ 11-8-2018Документ9 страницCREW Whitaker Recusal Letter DOJ 11-8-2018Beverly TranОценок пока нет
- Wipro Home Office RangeДокумент8 страницWipro Home Office RangePrashant RawatОценок пока нет
- The Biography of Hazrat Shah Qamaos Sahib in One PageДокумент3 страницыThe Biography of Hazrat Shah Qamaos Sahib in One PageMohammed Abdul Hafeez, B.Com., Hyderabad, IndiaОценок пока нет
- 10 Rules of Statcon by Atty Marcus NeelyДокумент4 страницы10 Rules of Statcon by Atty Marcus NeelyMorin OcoОценок пока нет
- Effectives of e Wallets NewДокумент15 страницEffectives of e Wallets NewRicardo SantosОценок пока нет
- Onechanbara - Bikini Samurai Squad Game GuideДокумент83 страницыOnechanbara - Bikini Samurai Squad Game GuideStefan RoscaОценок пока нет
- B.tech Cse Third Yr Syllabus 21-06-2018Документ21 страницаB.tech Cse Third Yr Syllabus 21-06-2018SuperdudeGauravОценок пока нет
- 5 Manifestos Da ArteДокумент3 страницы5 Manifestos Da ArteCinthia MendonçaОценок пока нет
- Natural Gas DistributionДокумент46 страницNatural Gas DistributionscribdmisraОценок пока нет
- Interview With Hohepa Mapiria Joseph - Joe - Murphy Royal Regent 7 July 2003Документ61 страницаInterview With Hohepa Mapiria Joseph - Joe - Murphy Royal Regent 7 July 2003kiwiit100% (8)
- Jobsheet PMДокумент49 страницJobsheet PMwindhy fitrianaОценок пока нет
- China Email ListДокумент3 страницыChina Email ListRosie Brown40% (5)