Вам также может понравиться
- Blood Chemistry and CBC Analysis - Clinical Laboratory Testing From A Functional Perspective - Quick Reference GuideДокумент29 страницBlood Chemistry and CBC Analysis - Clinical Laboratory Testing From A Functional Perspective - Quick Reference Guidejamesilluminare73% (15)
- Transfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaДокумент41 страницаTransfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaAETCM Emergency medicineОценок пока нет
- Chapter 4Документ29 страницChapter 4starykОценок пока нет
- Jcu 17 127 PDFДокумент8 страницJcu 17 127 PDFRezkyFYОценок пока нет
- Sharawey2011 PDFДокумент7 страницSharawey2011 PDFIkram DibОценок пока нет
- Relation Between Progression and Regression of ... Coronary Artery Disease and Serum Cholesterol LevelsДокумент19 страницRelation Between Progression and Regression of ... Coronary Artery Disease and Serum Cholesterol LevelsJОценок пока нет
- Arteriovenous Thrombosis in Chronic Renal Failure Patients Receiving Renal Replacement TherapyДокумент6 страницArteriovenous Thrombosis in Chronic Renal Failure Patients Receiving Renal Replacement TherapyMaya RustamОценок пока нет
- Ischemia-Modified Albumin Use As A Prognostic Factor in Coronary Bypass SurgeryДокумент5 страницIschemia-Modified Albumin Use As A Prognostic Factor in Coronary Bypass SurgerySarah KemalasariОценок пока нет
- Angina Pectoris in Patients With Aortic Stenosis and Normal Coronary Arteries - CirculationДокумент24 страницыAngina Pectoris in Patients With Aortic Stenosis and Normal Coronary Arteries - CirculationOscar F RojasОценок пока нет
- Journal 2Документ3 страницыJournal 2Anis Rita PratiwiОценок пока нет
- Abstracts / Atherosclerosis 252 (2016) E1 Ee196 E185Документ2 страницыAbstracts / Atherosclerosis 252 (2016) E1 Ee196 E185MaulОценок пока нет
- Relatia Dintre Arteroscleroza Si Colesterol SericДокумент7 страницRelatia Dintre Arteroscleroza Si Colesterol SericBeniamin BorotaОценок пока нет
- Impact of Albumin RL For BTДокумент10 страницImpact of Albumin RL For BTSandeep BhaskaranОценок пока нет
- Siadh vs. CSWДокумент6 страницSiadh vs. CSWFadiah Izzati SalimОценок пока нет
- Evaluation of Factors Affecting Liver Function Test in Patients Underwent Coronary Artery Bypass Graft SurgeryДокумент7 страницEvaluation of Factors Affecting Liver Function Test in Patients Underwent Coronary Artery Bypass Graft SurgeryajmrdОценок пока нет
- JURNALДокумент8 страницJURNALICHWANUDDINBUCHORIОценок пока нет
- Citrate in CRRTДокумент8 страницCitrate in CRRTAshish PandeyОценок пока нет
- Ojsadmin, 176Документ4 страницыOjsadmin, 176Signor 2019Оценок пока нет
- JASN SDHD Paper 2005Документ11 страницJASN SDHD Paper 2005Carlos EghiОценок пока нет
- Trombosit Dan D-Dimer (Inggris)Документ8 страницTrombosit Dan D-Dimer (Inggris)lidawatiОценок пока нет
- Rediana Murti N, Suryono, Jauhar FirdausДокумент6 страницRediana Murti N, Suryono, Jauhar Firdausrediana murti noviaОценок пока нет
- Fluid Resuscitation - Dita AditianingsihДокумент48 страницFluid Resuscitation - Dita AditianingsihGalih Wicaksono100% (1)
- Plasma Homocysteine and Total Thiol Content in Patients With Exudative Age-Related Macular DegenerationДокумент5 страницPlasma Homocysteine and Total Thiol Content in Patients With Exudative Age-Related Macular DegenerationAnonymous 1jCVqQuОценок пока нет
- Pathophysiology of COPDДокумент4 страницыPathophysiology of COPDrinieeeОценок пока нет
- Addison K May, MD John P Reilly, MD, Msce Scott Manaker, MD, PHD Arthur J Silvergleid, MD Geraldine Finlay, MD Contributor DisclosuresДокумент12 страницAddison K May, MD John P Reilly, MD, Msce Scott Manaker, MD, PHD Arthur J Silvergleid, MD Geraldine Finlay, MD Contributor DisclosuresAlvaro HaroОценок пока нет
- Original Article Coagulation Abnormalities in Patients With Chronic Liver Disease in PakistanДокумент5 страницOriginal Article Coagulation Abnormalities in Patients With Chronic Liver Disease in PakistanAsfandyar RoghaniОценок пока нет
- Cardio Resource UnitsДокумент31 страницаCardio Resource Unitsgraveheart11Оценок пока нет
- Stroke and LipidДокумент4 страницыStroke and LipidvenniariskiaОценок пока нет
- S64 FullДокумент3 страницыS64 FullkarenafiafiОценок пока нет
- Cardiorenal Syndrome: SciencedirectДокумент10 страницCardiorenal Syndrome: SciencedirectDwiFitriaAnggrainiОценок пока нет
- The Effect of Cilostazol On Right Heart FunctionДокумент43 страницыThe Effect of Cilostazol On Right Heart FunctionGunawan YogaОценок пока нет
- Cardiorenal SyndromeДокумент18 страницCardiorenal Syndromedauz3017Оценок пока нет
- 1 Hemofiltración RMH 1994Документ9 страниц1 Hemofiltración RMH 1994PILARICA201263Оценок пока нет
- Arterio-Venous Fistula Recirculation in Hemodialysis: Causes and PrevalencesДокумент8 страницArterio-Venous Fistula Recirculation in Hemodialysis: Causes and PrevalencesMashiur RahmanОценок пока нет
- 1 s2.0 073510979390668Q Main PDFДокумент9 страниц1 s2.0 073510979390668Q Main PDFPribac RamonaОценок пока нет
- Molecular Adsorbent Recirculating System and Single-Pass Albumin Dialysis in Liver Failure - A Prospective, Randomised Crossover StudyДокумент13 страницMolecular Adsorbent Recirculating System and Single-Pass Albumin Dialysis in Liver Failure - A Prospective, Randomised Crossover StudyRicardo RodriguezОценок пока нет
- 1757 7241 21 86Документ12 страниц1757 7241 21 86Nicco MarantsonОценок пока нет
- Acute Hypercalcemic Hypertension in Man: Role of Hemodynamics, Catecholamines, and ReninДокумент5 страницAcute Hypercalcemic Hypertension in Man: Role of Hemodynamics, Catecholamines, and ReninRo KohnОценок пока нет
- The Perindopril in Elderly PeopleДокумент8 страницThe Perindopril in Elderly PeopleluchititaОценок пока нет
- 8931 26614 2 PB PDFДокумент7 страниц8931 26614 2 PB PDFMaferОценок пока нет
- High Risk of Coagulopathy Among Type-2 Diabetes Mellitus Clients at A Municipal Hospital in GhanaДокумент7 страницHigh Risk of Coagulopathy Among Type-2 Diabetes Mellitus Clients at A Municipal Hospital in GhanaLovi AnaОценок пока нет
- Chiu 2016Документ7 страницChiu 2016alan arroyoОценок пока нет
- Jurnal Yang DipakeДокумент8 страницJurnal Yang DipakeEsy LОценок пока нет
- Syntax Score and Its Relation To Lipoprotein A - LP (A) and Extended Lipid Parameters in Non-Diabetic Patients With Acute Coronary Syndrome Having Age Below 55 YearsДокумент7 страницSyntax Score and Its Relation To Lipoprotein A - LP (A) and Extended Lipid Parameters in Non-Diabetic Patients With Acute Coronary Syndrome Having Age Below 55 YearsPremier PublishersОценок пока нет
- bb5 ClassifsofttissueДокумент5 страницbb5 ClassifsofttissueMuhammad MaulanaОценок пока нет
- Low Alt CKDДокумент5 страницLow Alt CKDFebianti RukmanaОценок пока нет
- QT Dispersion in Patients With Systemic Lupus Erythematosus: The Impact of Disease ActivityДокумент5 страницQT Dispersion in Patients With Systemic Lupus Erythematosus: The Impact of Disease ActivityWahyubudi PratamaОценок пока нет
- The Effect of Aerobic Exercise On Blood and Plasma Viscosity On Cardiac Health Club ParticipantsДокумент4 страницыThe Effect of Aerobic Exercise On Blood and Plasma Viscosity On Cardiac Health Club ParticipantsDedy SavradinataОценок пока нет
- Revisiting The Role of Oxygen Therapy in Cardiac Patients: Raman Moradkhan, MD, Lawrence I. Sinoway, MDДокумент4 страницыRevisiting The Role of Oxygen Therapy in Cardiac Patients: Raman Moradkhan, MD, Lawrence I. Sinoway, MDIda LemonОценок пока нет
- AnaemiaДокумент27 страницAnaemiaSamahir F HusseinОценок пока нет
- Hemodynamic Support in Fluid-Refractory Pediatric Septic ShockДокумент6 страницHemodynamic Support in Fluid-Refractory Pediatric Septic ShockJosé Pepo Apey ReinosoОценок пока нет
- Anemia and Thrombocytopenia in Acute and Chronic Renal Failure PDFДокумент6 страницAnemia and Thrombocytopenia in Acute and Chronic Renal Failure PDFSatriyo Dwi SuryantoroОценок пока нет
- Levosimendan in Perioperative Cardiothoracic Practice - A Narrative Review-FirstДокумент22 страницыLevosimendan in Perioperative Cardiothoracic Practice - A Narrative Review-FirstNehemias MD GuevaraОценок пока нет
- Mitrovic 2009Документ10 страницMitrovic 2009Lucas BragaОценок пока нет
- Bahan Referat Miocardial Stunning Perit Dial Int-2011-Selby-27-33Документ7 страницBahan Referat Miocardial Stunning Perit Dial Int-2011-Selby-27-33viniganorОценок пока нет
- A Randomized, Double Blind Comparison of Lactated.61Документ7 страницA Randomized, Double Blind Comparison of Lactated.61Temoc TemocОценок пока нет
- Comparison of The Plasma Levels of Apolipoproteins B and A-L, and Other Risk Factors in Men and Women With Premature Coronary Artery DiseaseДокумент7 страницComparison of The Plasma Levels of Apolipoproteins B and A-L, and Other Risk Factors in Men and Women With Premature Coronary Artery DiseaseCamilo HernándezОценок пока нет
- PIIS0016508597003843Документ8 страницPIIS0016508597003843Mudassar SattarОценок пока нет
- Shock Five Point ZeroДокумент78 страницShock Five Point ZeroprashsubbuОценок пока нет
- Alternatives to Blood Transfusion in Transfusion MedicineОт EverandAlternatives to Blood Transfusion in Transfusion MedicineAlice ManiatisОценок пока нет
- HDL PDFДокумент10 страницHDL PDFDiah Ayu AdiatiОценок пока нет
- CV MS 071209Документ5 страницCV MS 071209Diah Ayu AdiatiОценок пока нет
- Jurnal JantungДокумент11 страницJurnal JantungDiah Ayu AdiatiОценок пока нет
- Jurnal JantungДокумент9 страницJurnal JantungDiah Ayu AdiatiОценок пока нет
- Jurnal JantungДокумент10 страницJurnal JantungDiah Ayu AdiatiОценок пока нет
- Jurnal JantungДокумент11 страницJurnal JantungDiah Ayu AdiatiОценок пока нет
- Jurnal JantungДокумент14 страницJurnal JantungDiah Ayu AdiatiОценок пока нет
- Jurnal JantungДокумент7 страницJurnal JantungDiah Ayu AdiatiОценок пока нет
- Jurnal JantungДокумент11 страницJurnal JantungDiah Ayu AdiatiОценок пока нет
- Jurnal JantungДокумент7 страницJurnal JantungDiah Ayu AdiatiОценок пока нет
- SchizophreniaДокумент32 страницыSchizophreniaHerlina SihalohoОценок пока нет
- PJK JurnalДокумент4 страницыPJK JurnalDiah Ayu AdiatiОценок пока нет
- NeurotransmittersДокумент16 страницNeurotransmittersKiyomasa KatoОценок пока нет
- Corneal InfectionsДокумент8 страницCorneal InfectionsDiah Ayu AdiatiОценок пока нет
- JADASSmanagement Main PDFДокумент10 страницJADASSmanagement Main PDFPragatiОценок пока нет
- Nursing Practice IvДокумент24 страницыNursing Practice IvJohn wewОценок пока нет
- Gonad in The BodyДокумент10 страницGonad in The Bodyjuliana leonОценок пока нет
- Catecholamines and The Effects of Exercise, Training and GenderДокумент24 страницыCatecholamines and The Effects of Exercise, Training and GenderMenna Tesfaye MigbarОценок пока нет
- Group 2 Culture TechniqueДокумент38 страницGroup 2 Culture TechniqueBartazal dawaganОценок пока нет
- Digoxin Drug CardДокумент1 страницаDigoxin Drug CardMahsa Ahmadzadeh100% (2)
- Metabolic AlkalosisДокумент15 страницMetabolic AlkalosisMenna ElesawyОценок пока нет
- Nama BHP & Kode Barang Lab EkadaДокумент3 страницыNama BHP & Kode Barang Lab EkadaPipit latuОценок пока нет
- Lact2 2018-11 v12Документ4 страницыLact2 2018-11 v12Kouame FrancisОценок пока нет
- Infographic Folic Acid Vs FolateДокумент1 страницаInfographic Folic Acid Vs FolateKaterina PoposkaОценок пока нет
- 2021 Article 1063Документ15 страниц2021 Article 1063Raúl LópezОценок пока нет
- Lipid Catabolism: Overview of Lipid MetabolismДокумент3 страницыLipid Catabolism: Overview of Lipid Metabolismninafatima allamОценок пока нет
- Review of Digestion MetabolismДокумент4 страницыReview of Digestion MetabolismAntonia SalvadorОценок пока нет
- Efeito Browning Nos Adipócitos ApostilaДокумент31 страницаEfeito Browning Nos Adipócitos ApostilaRachel RodriguesОценок пока нет
- Adrenal Gland - Physiology, Pathology, and Pharmacology - Lecturio PDFДокумент8 страницAdrenal Gland - Physiology, Pathology, and Pharmacology - Lecturio PDFfaiz alamОценок пока нет
- 1700 Mock 2 PDFДокумент37 страниц1700 Mock 2 PDFSiraj Ul IslamОценок пока нет
- Male Reproductive SystemДокумент9 страницMale Reproductive SystemSarilyn Simon50% (2)
- John K. Mathai, Yanhong Liu and Hans H. SteinДокумент10 страницJohn K. Mathai, Yanhong Liu and Hans H. SteinDébora Giaretta ZattaОценок пока нет
- Bahasa Inggris 1.13Документ5 страницBahasa Inggris 1.13Rizky AdiОценок пока нет
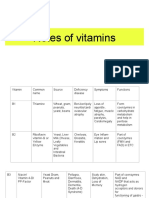
- Notes of VitaminsДокумент8 страницNotes of VitaminsEllyОценок пока нет
- Ang Tunay Na Excretory SystemДокумент17 страницAng Tunay Na Excretory SystemcjОценок пока нет
- GravoiДокумент6 страницGravoiPam Barboza100% (1)
- Week 6-7 - Environmental Health and ToxicologyДокумент33 страницыWeek 6-7 - Environmental Health and ToxicologyLorenz GarciaОценок пока нет
- Filesugd66484b .PDF 2Документ75 страницFilesugd66484b .PDF 2صاحب القلمОценок пока нет
- Endocrine SystemДокумент11 страницEndocrine Systemshannon c. lewisОценок пока нет
- Biology (Zoology, Botany, Health), Environment & AgricultureДокумент1 страницаBiology (Zoology, Botany, Health), Environment & AgriculturerjtbtbtbОценок пока нет
- A Wearable Electrochemical Biosensor For The Monitoring of Metabolites and NutrientsДокумент13 страницA Wearable Electrochemical Biosensor For The Monitoring of Metabolites and NutrientsBAUTISTA DIPAOLA100% (1)
- Notes For PediatricsДокумент38 страницNotes For PediatricsadamsamillionОценок пока нет