Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- IOSH Managing Safely V5.0 Project Template (Risk Assessment Form)Документ3 страницыIOSH Managing Safely V5.0 Project Template (Risk Assessment Form)Dimitar GeorgievОценок пока нет
- Farmacist Desk Reference ReviewДокумент1 страницаFarmacist Desk Reference ReviewThinh DoОценок пока нет
- Antenatal Assessment - Case No-1Документ4 страницыAntenatal Assessment - Case No-1Prity DeviОценок пока нет
- The Prevention and Management of Pressure UlcerДокумент5 страницThe Prevention and Management of Pressure UlcerrantiОценок пока нет
- Cardiology BrochureДокумент2 страницыCardiology Brochureong251183Оценок пока нет
- Root Dilaceration: A Case Report and Literature ReviewДокумент11 страницRoot Dilaceration: A Case Report and Literature ReviewAstrid HutabaratОценок пока нет
- Required Coursework For Dental SchoolДокумент5 страницRequired Coursework For Dental Schoolrqaeibifg100% (2)
- Rajiv Gandhi University of Health Sciences Exam ResultДокумент1 страницаRajiv Gandhi University of Health Sciences Exam ResultMD ZubairОценок пока нет
- FPSC Charge Nurse Result 27 Sep 2019 PDFДокумент19 страницFPSC Charge Nurse Result 27 Sep 2019 PDFUmairОценок пока нет
- Interproximal Enamel Reduction As A Part of Orthodontic TreatmentДокумент6 страницInterproximal Enamel Reduction As A Part of Orthodontic Treatmentdrgeorgejose7818Оценок пока нет
- Community Health NursingДокумент10 страницCommunity Health NursingChristiane BautistaОценок пока нет
- 2021 CPT CodesДокумент8 страниц2021 CPT CodesSundar RamanathanОценок пока нет
- Vis AnneДокумент22 страницыVis AnneImelda AtikaОценок пока нет
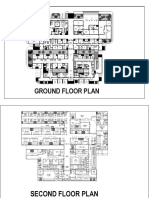
- Sample Plan HospitalДокумент3 страницыSample Plan HospitalMarkNova100% (1)
- Part 1 - Curriculum VitaeДокумент33 страницыPart 1 - Curriculum VitaeAmriatiОценок пока нет
- SickLeaveCertificate With and Without Diagnosis 20240227 144109Документ2 страницыSickLeaveCertificate With and Without Diagnosis 20240227 144109Sawad SawaОценок пока нет
- Rating Criteria: Prior To Woman'S Transfer To The DRДокумент3 страницыRating Criteria: Prior To Woman'S Transfer To The DRPatricia Ann JaringОценок пока нет
- Test Bank For Health Psychology 2 e 2nd Edition Deborah Fish RaginДокумент34 страницыTest Bank For Health Psychology 2 e 2nd Edition Deborah Fish RaginpudgyoverburnnggОценок пока нет
- MedicalCertificate ExmpleДокумент1 страницаMedicalCertificate ExmpleJareena SamsonОценок пока нет
- CyclosporineДокумент3 страницыCyclosporineraki9999Оценок пока нет
- Probiotics Downloadable PDFДокумент2 страницыProbiotics Downloadable PDFGreg WrightОценок пока нет
- KENDRIYA VIDYALAYA Biology Investigatory ProjectДокумент28 страницKENDRIYA VIDYALAYA Biology Investigatory Projectvishali GОценок пока нет
- Pressure Points - Postnatal Care Planning PDFДокумент15 страницPressure Points - Postnatal Care Planning PDFNoraОценок пока нет
- Dentinal HypersensitivityДокумент11 страницDentinal HypersensitivityAmira KaddouОценок пока нет
- Isaac Banda-MPH 2012 DissertationДокумент60 страницIsaac Banda-MPH 2012 DissertationmalikmanОценок пока нет
- ProductsДокумент65 страницProductsanooprajguruОценок пока нет
- DM Brochure For NCM 106Документ12 страницDM Brochure For NCM 106Kimsha ConcepcionОценок пока нет
- Primary Survey & Secondary Survey: Presentor: Shellazianne Anak Ringam Date: 20 November 2015Документ27 страницPrimary Survey & Secondary Survey: Presentor: Shellazianne Anak Ringam Date: 20 November 2015Keluang Man WinchesterОценок пока нет
- Various Face Bow Transfer TechniquesДокумент49 страницVarious Face Bow Transfer TechniquesDr.Sathyabhama A.V100% (1)
- Postpartum Depression Theory (译)Документ5 страницPostpartum Depression Theory (译)彭钰莹Оценок пока нет