Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Wound Ostomy Continence Skills ChecklistДокумент4 страницыWound Ostomy Continence Skills ChecklistnorthweststaffingОценок пока нет
- Curative and Rehabilitative Nursing Care Management of Clients in Acute Biologic CrisisДокумент44 страницыCurative and Rehabilitative Nursing Care Management of Clients in Acute Biologic CrisisArgee AlonsabeОценок пока нет
- A Case Study On SchizophreniaДокумент11 страницA Case Study On SchizophreniaRosa Isabel57% (7)
- The Attitudes and Beliefs About Over-the-Counter MedicinesДокумент4 страницыThe Attitudes and Beliefs About Over-the-Counter MedicinesMahendra AvinashОценок пока нет
- Lesson 12 - Overview of The Wastewater Treatment ProcessДокумент6 страницLesson 12 - Overview of The Wastewater Treatment ProcessZar ChiОценок пока нет
- Nursereview Org Therapeutic Communication TechniquesДокумент6 страницNursereview Org Therapeutic Communication TechniquesPatricia VasquezОценок пока нет
- The Maximization of Exposure TherapyДокумент12 страницThe Maximization of Exposure TherapyAuroraОценок пока нет
- Patient Profile Data Form: Advance DirectivesДокумент6 страницPatient Profile Data Form: Advance DirectivesMa Cecilia SorianoОценок пока нет
- Multidimensional Family Therapy - Working With AdolescentsДокумент7 страницMultidimensional Family Therapy - Working With AdolescentsLen PetersОценок пока нет
- Endodontic Clinic Manual 2015 - 1Документ134 страницыEndodontic Clinic Manual 2015 - 1Adina Popa100% (2)
- 11.efficacy and Stability of The Alar Base Cinch SutureДокумент4 страницы11.efficacy and Stability of The Alar Base Cinch SutureFabian Camelo OtorrinoОценок пока нет
- CBD Sirosis, Hematemesis MelenaДокумент29 страницCBD Sirosis, Hematemesis Melenadyah farahОценок пока нет
- Why Are Black Women Rated Less Physically Attractive Than Other Women, But Black Men Are Rated Better Looking Than Other Men?Документ6 страницWhy Are Black Women Rated Less Physically Attractive Than Other Women, But Black Men Are Rated Better Looking Than Other Men?koa_x100% (2)
- Epilepsy 2015 A Practical Guide PDFДокумент283 страницыEpilepsy 2015 A Practical Guide PDFrahma100% (1)
- Techniques of MassageДокумент1 страницаTechniques of MassageVladGrosuОценок пока нет
- Medical Device PackagingДокумент17 страницMedical Device Packaging049 Nishigandha NadavadeОценок пока нет
- Cancer (Medical Term:Malignant NeoplasmДокумент7 страницCancer (Medical Term:Malignant NeoplasmolussojiОценок пока нет
- Osteoporosis and Fragility Fractures Surgical PerpspectiveДокумент54 страницыOsteoporosis and Fragility Fractures Surgical PerpspectiveSonal DudaniОценок пока нет
- First Aid Cdrrmo 2019Документ373 страницыFirst Aid Cdrrmo 2019fenan sollanoОценок пока нет
- Strength and Conditioning Coach or Sports Performance Coach or FДокумент3 страницыStrength and Conditioning Coach or Sports Performance Coach or Fapi-121340325Оценок пока нет
- McNamee 1996 Therapy and IdentityДокумент16 страницMcNamee 1996 Therapy and IdentityPsic Karina BautistaОценок пока нет
- Topical AntifungalsДокумент14 страницTopical AntifungalsRasha Mohammad100% (1)
- Bad Ragaz Ring MethodДокумент22 страницыBad Ragaz Ring MethodNurdina Afini0% (1)
- Movement Diagrams - Rayner & Smale PDFДокумент6 страницMovement Diagrams - Rayner & Smale PDFItai IzhakОценок пока нет
- BAUTISTA, DYANNE G. - Oncology Nursing Colorectal Cancer Case StudyДокумент16 страницBAUTISTA, DYANNE G. - Oncology Nursing Colorectal Cancer Case StudyDyanne BautistaОценок пока нет
- Burnout - Existential Meaning and Possibilities of Prevention (Alfried Längle)Документ16 страницBurnout - Existential Meaning and Possibilities of Prevention (Alfried Längle)abaeram2Оценок пока нет
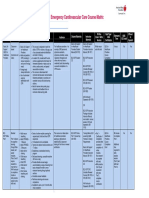
- Emergency Cardiovascular Care Course MatrixДокумент15 страницEmergency Cardiovascular Care Course MatrixJesus M. Espinosa EchavarriaОценок пока нет
- MDS Oral Medicine Question Papers 2002Документ5 страницMDS Oral Medicine Question Papers 2002Niyas UmmerОценок пока нет
- CBT For Panic DisorderДокумент40 страницCBT For Panic Disordersavvy_as_98100% (1)
- Pharm Cal-Revised Green PDFДокумент15 страницPharm Cal-Revised Green PDFSheila May ChiongОценок пока нет