Вам также может понравиться
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- PleuraFlow Brochure ML004 I FINALДокумент4 страницыPleuraFlow Brochure ML004 I FINALxergiogcОценок пока нет
- Reconstruction of Mandible Using A Computer-Designed 3d-Printed Patient-Specific Titanium Implant: A Case ReportДокумент9 страницReconstruction of Mandible Using A Computer-Designed 3d-Printed Patient-Specific Titanium Implant: A Case ReportExo AnubisОценок пока нет
- Flap Design and Mandibularthird Molar Surgery A Splitmouth Randomized Clinical StudyДокумент5 страницFlap Design and Mandibularthird Molar Surgery A Splitmouth Randomized Clinical StudyFatima SiddiquiОценок пока нет
- Closure of Paediatric Tracheocutaneous Fistula - Surgical TechniqueДокумент6 страницClosure of Paediatric Tracheocutaneous Fistula - Surgical Techniquehai1Оценок пока нет
- IPSGДокумент4 страницыIPSGmohsinaОценок пока нет
- Basic Life Support: Practice Test QuestionsДокумент6 страницBasic Life Support: Practice Test QuestionsDay Moreno100% (3)
- Carboxyl Methyl CelluloseДокумент19 страницCarboxyl Methyl CelluloseJamatul FirdausОценок пока нет
- Chapter 11. Cardiovascular-SystemДокумент10 страницChapter 11. Cardiovascular-SystemScianna Christel LastimosaОценок пока нет
- CGHS Pune Rates 2018Документ44 страницыCGHS Pune Rates 2018N.J. WaghmareОценок пока нет
- Instruments Extra Ocular PDFДокумент38 страницInstruments Extra Ocular PDFrajmalhotra167Оценок пока нет
- Case Report - MyopathyДокумент17 страницCase Report - MyopathydewaОценок пока нет
- Osteology and Gluteal Region TransДокумент18 страницOsteology and Gluteal Region Transchynne ongОценок пока нет
- CT-based Diagnostic Algorithm To Identify Bowel and or MesentericДокумент10 страницCT-based Diagnostic Algorithm To Identify Bowel and or Mesenteric林耿毅Оценок пока нет
- Gastrointestinal BleedingДокумент31 страницаGastrointestinal BleedingDenice IsidroОценок пока нет
- 2019 Guidelines Bariatric Surgery EAES SAGESДокумент29 страниц2019 Guidelines Bariatric Surgery EAES SAGESDra Maha HafezОценок пока нет
- Human Skeletal System PPTДокумент73 страницыHuman Skeletal System PPTInsatiable CleeОценок пока нет
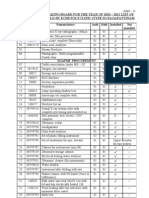
- Annual Stock Taking Board For The Year of 2010 - 2011 List of Maj Med Eqpt-Held by Echs Polyclinic (Type-D) NagapattinamДокумент17 страницAnnual Stock Taking Board For The Year of 2010 - 2011 List of Maj Med Eqpt-Held by Echs Polyclinic (Type-D) NagapattinamechsngtОценок пока нет
- Annotated Bibliography FinalДокумент15 страницAnnotated Bibliography Finaledetrez94Оценок пока нет
- Acute CholangitisДокумент9 страницAcute CholangitisMike GОценок пока нет
- BBraun Vet SuturesДокумент91 страницаBBraun Vet SuturesAlex ZakutashviliОценок пока нет
- NEET SS 2017 ResultДокумент24 страницыNEET SS 2017 ResultabhaymalurОценок пока нет
- Basic Life Support PresentationДокумент34 страницыBasic Life Support PresentationMona ElhassanОценок пока нет
- Managing Abruptio Placentae: An EmergencyДокумент23 страницыManaging Abruptio Placentae: An EmergencySharoon KumarОценок пока нет
- Organizing Neonatal CareДокумент17 страницOrganizing Neonatal CareManisha ThakurОценок пока нет
- South Africa Licensed Ectromedical Devices ListДокумент281 страницаSouth Africa Licensed Ectromedical Devices ListAbdullah MuhammadОценок пока нет
- RPT 54Документ50 страницRPT 54Leticia LopezОценок пока нет
- Advanced Paediatric Life Support - A0 PDFДокумент1 страницаAdvanced Paediatric Life Support - A0 PDFiulia-uroОценок пока нет
- 9 1 EndosДокумент6 страниц9 1 EndosmghОценок пока нет
- Moderator - DR Prof. R.K. Bundela Presented by - Dr. Mohd Raza .Документ44 страницыModerator - DR Prof. R.K. Bundela Presented by - Dr. Mohd Raza .alpana100% (1)
- D2 Gastrectomy: DR K Suneel Kaushik Senior Resident Surgical OncologyДокумент66 страницD2 Gastrectomy: DR K Suneel Kaushik Senior Resident Surgical OncologySuneel Kaushik KОценок пока нет