Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Organizational Chart Tertiary LabДокумент1 страницаOrganizational Chart Tertiary LabMiki Nishihara86% (7)
- Problems: 4: The Aminoglycoside AntibioticsДокумент3 страницыProblems: 4: The Aminoglycoside AntibioticsSaul RuizОценок пока нет
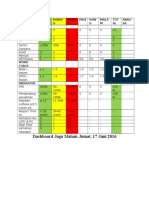
- Dashboard Jaga Malam Jumat, 17 Juni 2016: Uraian Hijau Kunin G Mera H Pagi Sian G Mala M TOT AL Anali SA AktifitasДокумент4 страницыDashboard Jaga Malam Jumat, 17 Juni 2016: Uraian Hijau Kunin G Mera H Pagi Sian G Mala M TOT AL Anali SA AktifitasNurLatifah Chairil AnwarОценок пока нет
- Jurnal TBC Pada AnakДокумент6 страницJurnal TBC Pada AnakAlfi RahmanОценок пока нет
- Fluffy Japanese PancakesДокумент3 страницыFluffy Japanese PancakesNurLatifah Chairil AnwarОценок пока нет
- Definition of PregnancyДокумент9 страницDefinition of PregnancyNurLatifah Chairil AnwarОценок пока нет
- HEMOROIDДокумент5 страницHEMOROIDNurLatifah Chairil AnwarОценок пока нет
- Intoxication Case Analysis: Dra. Suhartini, Apt., SU Dr. Idha Arfianti MSCДокумент19 страницIntoxication Case Analysis: Dra. Suhartini, Apt., SU Dr. Idha Arfianti MSCNurLatifah Chairil AnwarОценок пока нет
- Trends in Anasthesia and Critical CareДокумент6 страницTrends in Anasthesia and Critical CareNurLatifah Chairil AnwarОценок пока нет
- Shock ManagementДокумент12 страницShock ManagementNurLatifah Chairil Anwar100% (1)
- Pediatrics Stones JAMA Peds 2015Документ7 страницPediatrics Stones JAMA Peds 2015NurLatifah Chairil AnwarОценок пока нет
- Varicella Zoster Virus OpthalmicusДокумент10 страницVaricella Zoster Virus OpthalmicusNurLatifah Chairil AnwarОценок пока нет
- The Liability of Anasthesiologist in Ambulatory SurgeryДокумент7 страницThe Liability of Anasthesiologist in Ambulatory SurgeryNurLatifah Chairil AnwarОценок пока нет
- Jurnal Atopic Dermatitis: Dokter Pembimbing: Dr. Eko Krisnarto, SP - KK Disusun Oleh Nurlatifah Chairil Anwar (406151030)Документ5 страницJurnal Atopic Dermatitis: Dokter Pembimbing: Dr. Eko Krisnarto, SP - KK Disusun Oleh Nurlatifah Chairil Anwar (406151030)NurLatifah Chairil AnwarОценок пока нет
- Microbiology of WoundsДокумент31 страницаMicrobiology of WoundsintanpurnОценок пока нет
- What Is Art DecoДокумент3 страницыWhat Is Art DecoNurLatifah Chairil AnwarОценок пока нет
- Abs TrakДокумент3 страницыAbs TrakNurLatifah Chairil AnwarОценок пока нет
- Hospital 2Документ3 страницыHospital 2PRIYAM XEROXОценок пока нет
- Case Study C-Section PatientДокумент21 страницаCase Study C-Section Patientapi-458907281100% (1)
- Activity 5 TitrationДокумент1 страницаActivity 5 TitrationPorcha PacsayОценок пока нет
- Medication Card AncefДокумент2 страницыMedication Card AncefEllieОценок пока нет
- Ballad Scarce Resource Allocation Patient Notification LetterДокумент2 страницыBallad Scarce Resource Allocation Patient Notification LetterJosh Smith100% (1)
- Ama Report of The Council On Science and Public Health Obesity As A DiseaseДокумент14 страницAma Report of The Council On Science and Public Health Obesity As A Diseaseapi-285790500Оценок пока нет
- Sound Treatement Case Study - Operating TheatreДокумент1 страницаSound Treatement Case Study - Operating TheatreSaint-Gobain Ecophon (UK)Оценок пока нет
- Oral and Dental Aspects of Child Abuse: GoogleДокумент48 страницOral and Dental Aspects of Child Abuse: GoogleZuhrah Vitri YatiОценок пока нет
- 12 The Changing Face of Aesthetic DentistryДокумент8 страниц12 The Changing Face of Aesthetic DentistryOziel Ramirez OrtegaОценок пока нет
- Basics For IV PreparationДокумент46 страницBasics For IV PreparationOmayma IzzeldinОценок пока нет
- Overview of The Philippine Health SystemДокумент10 страницOverview of The Philippine Health SystemCaryl Ann RabanosОценок пока нет
- Kenyatta National Hospital Internship ReДокумент33 страницыKenyatta National Hospital Internship Relex tecОценок пока нет
- Write More Examples of The Following ExpressionsДокумент2 страницыWrite More Examples of The Following ExpressionsS DestrianaОценок пока нет
- Referat ObsgynДокумент21 страницаReferat ObsgynRoberto HutapeaОценок пока нет
- Erythema Multiforme and HomoeopathyДокумент7 страницErythema Multiforme and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Health Problems Vocabulary Esl Matching Exercise Worksheet For KidsДокумент2 страницыHealth Problems Vocabulary Esl Matching Exercise Worksheet For KidsIsabel100% (1)
- 2018 @dentallib Douglas Deporter Short and Ultra Short ImplantsДокумент170 страниц2018 @dentallib Douglas Deporter Short and Ultra Short Implantsilter burak köseОценок пока нет
- Dip HIV Man (SA) Regulations 21 3 2020 PDFДокумент8 страницDip HIV Man (SA) Regulations 21 3 2020 PDFdchunОценок пока нет
- QuestionnaireДокумент6 страницQuestionnaireRyan DaetОценок пока нет
- Etextbook 978 1451187908 Maternal and Child Health Nursing Care of The Childbearing and Childrearing FamilyДокумент61 страницаEtextbook 978 1451187908 Maternal and Child Health Nursing Care of The Childbearing and Childrearing Familyroger.newton507100% (48)
- Executive Order No. 003-AДокумент2 страницыExecutive Order No. 003-AAndrew Murray D. DuranoОценок пока нет
- Ethnomedicine and Drug Discovery PDFДокумент2 страницыEthnomedicine and Drug Discovery PDFJohn0% (1)
- PIIS0015028219324847Документ18 страницPIIS0015028219324847Maged BedeawyОценок пока нет
- Access To Childbirth CareДокумент67 страницAccess To Childbirth CareemeОценок пока нет
- Wrong Site Wrong ProcedureДокумент9 страницWrong Site Wrong ProcedureYohanes SusantoОценок пока нет
- Pyogenic GranulomaДокумент13 страницPyogenic GranulomaPiyusha SharmaОценок пока нет
- Nanda - Noc - Nic (NNN) : Intervensi KeperawatanДокумент39 страницNanda - Noc - Nic (NNN) : Intervensi KeperawatanChindy Surya KencanabreОценок пока нет
- Herbal Medicine For Treatment and Prevention of Liver DiseasesДокумент6 страницHerbal Medicine For Treatment and Prevention of Liver Diseaseskartini ciatawiОценок пока нет