Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Flow Chart - QCДокумент2 страницыFlow Chart - QCKarthikeyan Shanmugavel100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Dawn of Solar PV CookingДокумент5 страницDawn of Solar PV CookingAbhinav AgrawalОценок пока нет
- Tesla Coil ProjectДокумент8 страницTesla Coil ProjectShivam singhОценок пока нет
- Cecilia-Puff-Tee-Final-OUSM-Designs-12 MESES A TALLA 8Документ19 страницCecilia-Puff-Tee-Final-OUSM-Designs-12 MESES A TALLA 8Jose SanchezОценок пока нет
- Nasal ObstructionДокумент6 страницNasal Obstructionjoal510Оценок пока нет
- Eye in Facial ParalysisДокумент8 страницEye in Facial Paralysisjoal510Оценок пока нет
- Skin CancerДокумент35 страницSkin Cancerjoal510Оценок пока нет
- Ear InfectionsДокумент16 страницEar Infectionsjoal510Оценок пока нет
- ConjuntivitisДокумент21 страницаConjuntivitisjoal510Оценок пока нет
- Penetranting Cardiac InjuriesДокумент16 страницPenetranting Cardiac Injuriesjoal510Оценок пока нет
- Mandibulasr Truma ManagementДокумент18 страницMandibulasr Truma Managementjoal510Оценок пока нет
- Resumen: Funtional Abdominal Pain - PathogenesisДокумент17 страницResumen: Funtional Abdominal Pain - Pathogenesisjoal510Оценок пока нет
- 2006 129 1344-1348 Christopher E. Brightling: Clinical Applications of Induced SputumДокумент7 страниц2006 129 1344-1348 Christopher E. Brightling: Clinical Applications of Induced Sputumjoal510Оценок пока нет
- The Passion For Cacti and Other Succulents: June 2017Документ140 страницThe Passion For Cacti and Other Succulents: June 2017golf2010Оценок пока нет
- SP Essay 1Документ14 страницSP Essay 1api-511870420Оценок пока нет
- Health Promotion Throughout The Life Span 7th Edition Edelman Test BankДокумент35 страницHealth Promotion Throughout The Life Span 7th Edition Edelman Test Bankcourtneyharrisbpfyrkateq100% (17)
- SambongДокумент3 страницыSambongNica Del GallegoОценок пока нет
- PPT DIARHEA IN CHILDRENДокумент31 страницаPPT DIARHEA IN CHILDRENRifka AnisaОценок пока нет
- Lecture 12Документ8 страницLecture 12Mechanical ZombieОценок пока нет
- EPCC Hydrocarbon Downstream L&T 09.01.2014Документ49 страницEPCC Hydrocarbon Downstream L&T 09.01.2014shyaminannnaОценок пока нет
- 123 09-Printable Menu VORДокумент2 страницы123 09-Printable Menu VORArmstrong TowerОценок пока нет
- Nissan Copper LTDДокумент11 страницNissan Copper LTDankit_shahОценок пока нет
- Significance of GodboleДокумент5 страницSignificance of GodbolehickeyvОценок пока нет
- Module-4 (PDFDrive)Документ67 страницModule-4 (PDFDrive)Divya priya KОценок пока нет
- Semi Finals in Tle 2015Документ3 страницыSemi Finals in Tle 2015LoraineTenorioОценок пока нет
- Technical Information: Range-Free Controller FA-M3 System Upgrade GuideДокумент33 страницыTechnical Information: Range-Free Controller FA-M3 System Upgrade GuideAddaОценок пока нет
- G.S 5Документ2 страницыG.S 5Jamsher BalochОценок пока нет
- IV. Network Modeling, Simple SystemДокумент16 страницIV. Network Modeling, Simple SystemJaya BayuОценок пока нет
- Ali Erdemir: Professional ExperienceДокумент3 страницыAli Erdemir: Professional ExperienceDunkMeОценок пока нет
- Shandong Baoshida Cable Co, LTD.: Technical ParameterДокумент3 страницыShandong Baoshida Cable Co, LTD.: Technical ParameterkmiqdОценок пока нет
- Main Girders: CrossДокумент3 страницыMain Girders: Crossmn4webОценок пока нет
- AKI in ChildrenДокумент43 страницыAKI in ChildrenYonas AwgichewОценок пока нет
- TreesДокумент69 страницTreesADITYA GEHLAWATОценок пока нет
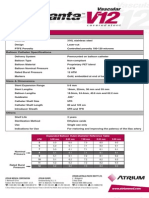
- Advanta V12 Data SheetДокумент2 страницыAdvanta V12 Data SheetJuliana MiyagiОценок пока нет
- DR PDFДокумент252 страницыDR PDFa_ouchar0% (1)
- SPL Lab Report3Документ49 страницSPL Lab Report3nadif hasan purnoОценок пока нет
- Presentation On 4G TechnologyДокумент23 страницыPresentation On 4G TechnologyFresh EpicОценок пока нет
- Murata High Voltage CeramicДокумент38 страницMurata High Voltage CeramictycristinaОценок пока нет
- Gypsum Plasterboard: National Standard of The People'S Republic of ChinaДокумент15 страницGypsum Plasterboard: National Standard of The People'S Republic of ChinaGarry100% (2)