Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Antibiotic Study Cheat Sheet August 2019Документ1 страницаAntibiotic Study Cheat Sheet August 2019Ryan TurnerОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Beta Lactam AntibioticsДокумент28 страницBeta Lactam AntibioticsHassan.shehri100% (11)
- Hospital-Acquired Pneumonia: Pathophysiology, Diagnosis, and TreatmentДокумент23 страницыHospital-Acquired Pneumonia: Pathophysiology, Diagnosis, and Treatmentdarmarianto100% (1)
- Infectious Disease - Antibiotic Ladder PDFДокумент2 страницыInfectious Disease - Antibiotic Ladder PDFVaishali PrasharОценок пока нет
- Major functions of adrenergic and cholinergic receptorsДокумент77 страницMajor functions of adrenergic and cholinergic receptorsBetsy Brown Byersmith100% (1)
- Print Antibiotics ReviewДокумент6 страницPrint Antibiotics ReviewtiuwangОценок пока нет
- Ventilator Associated Pneumonia TreatmentДокумент43 страницыVentilator Associated Pneumonia Treatmentmkc71Оценок пока нет
- GDP Europa 2016 1 28022018 BP enДокумент8 страницGDP Europa 2016 1 28022018 BP enyatedigo958Оценок пока нет
- Rates of Blood Cultures Positive For Vancomycin-Resistant: Enterococcus in Ontario: A Quasi-Experimental StudyДокумент8 страницRates of Blood Cultures Positive For Vancomycin-Resistant: Enterococcus in Ontario: A Quasi-Experimental Studyyatedigo958Оценок пока нет
- Mrsa MortalityДокумент16 страницMrsa Mortalityyatedigo958Оценок пока нет
- 1471 2334 12 83Документ10 страниц1471 2334 12 83yatedigo958Оценок пока нет
- ABC ECG - Myocardial IschaemiaДокумент5 страницABC ECG - Myocardial IschaemiaHanna_RОценок пока нет
- Empirical Therapy For Diabetic Foot InfectionsДокумент3 страницыEmpirical Therapy For Diabetic Foot Infectionsyatedigo958Оценок пока нет
- Isolation of Carbapenem-Resistant Pseudomonas Spp. From FoodДокумент6 страницIsolation of Carbapenem-Resistant Pseudomonas Spp. From FoodValentina RondonОценок пока нет
- Intrathecal Antibacterial and Antifungal TherapiesДокумент24 страницыIntrathecal Antibacterial and Antifungal TherapiesntnquynhproОценок пока нет
- Acute Complicated Urinary Tract Infection (Including Pyelonephritis) in Adults - UpToDateДокумент39 страницAcute Complicated Urinary Tract Infection (Including Pyelonephritis) in Adults - UpToDateLaís FialhoОценок пока нет
- Journal - Antimicrobial ResistanceДокумент12 страницJournal - Antimicrobial ResistanceTriLightОценок пока нет
- Antibiotic Cross-Sensitivity ChartДокумент1 страницаAntibiotic Cross-Sensitivity ChartChing JuОценок пока нет
- Risk Factors of Urinary Tract Infection Caused by Extended SpectrumДокумент5 страницRisk Factors of Urinary Tract Infection Caused by Extended SpectrumPrimasari DiahОценок пока нет
- Antibiotics: Review of Ceftazidime-Avibactam For The Treatment of Infections Caused by Pseudomonas AeruginosaДокумент24 страницыAntibiotics: Review of Ceftazidime-Avibactam For The Treatment of Infections Caused by Pseudomonas AeruginosaVictor Hugo SilveiraОценок пока нет
- Unedited Trs 2019 Ec22 SeptДокумент330 страницUnedited Trs 2019 Ec22 SeptTeddyОценок пока нет
- Urological Infections 2010.PDF EditДокумент112 страницUrological Infections 2010.PDF EditMuhammad Bilal Bin AmirОценок пока нет
- 10-Article Text-26-1-10-20170412Документ5 страниц10-Article Text-26-1-10-20170412naeem186Оценок пока нет
- Pediatric Community Acquired Pneumonia Treatment GuidelinesДокумент22 страницыPediatric Community Acquired Pneumonia Treatment GuidelinesJeanne Mae Lee AfallaОценок пока нет
- Analysis of Blood Culture Profile and Factors Related To Microbial Patterns and Antibiotic Resistance in Intensive Care UnitДокумент6 страницAnalysis of Blood Culture Profile and Factors Related To Microbial Patterns and Antibiotic Resistance in Intensive Care UnitInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- EUCAST Detection of Resistance Mechanisms 170711Документ43 страницыEUCAST Detection of Resistance Mechanisms 170711bicemanОценок пока нет
- IWGDF Guidelines on PAD ManagementДокумент47 страницIWGDF Guidelines on PAD ManagementSidan EmozieОценок пока нет
- MeropenemДокумент3 страницыMeropenemPuji Yunisyah RahayuОценок пока нет
- Antibiotics: Mechanisms, Classes, and Key DrugsДокумент7 страницAntibiotics: Mechanisms, Classes, and Key DrugsWendy EscalanteОценок пока нет
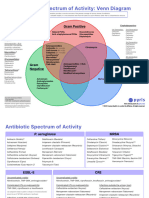
- Antibotics Venn DiagramДокумент2 страницыAntibotics Venn DiagramTop VidsОценок пока нет
- Detection of Beta LactamДокумент18 страницDetection of Beta LactamRajkishor YadavОценок пока нет
- Curs Engleza 2014 PDFДокумент263 страницыCurs Engleza 2014 PDFDeea TrancăОценок пока нет
- Formulation Stabilisation and Encapsulation of Bacteriophage For Phage TherapyДокумент34 страницыFormulation Stabilisation and Encapsulation of Bacteriophage For Phage TherapyGerman GodiОценок пока нет
- Overview of Antimicrobial Resistance - An Emerging Silent PandemicДокумент13 страницOverview of Antimicrobial Resistance - An Emerging Silent PandemicAbbireddy SairamОценок пока нет
- CMR 00047-19Документ37 страницCMR 00047-19UisanimgggОценок пока нет
- Extended Spectrum Beta Lactamase (Esbl) Production Among Enterobacteriaceae in A Tertiary Care CentreДокумент10 страницExtended Spectrum Beta Lactamase (Esbl) Production Among Enterobacteriaceae in A Tertiary Care CentreVadivel N P PillaiОценок пока нет