Вам также может понравиться
- Fertility: Meal PlanДокумент17 страницFertility: Meal PlanDwi Ayu KusumawardaniОценок пока нет
- Jurnal 1 MenopauseДокумент7 страницJurnal 1 MenopauseWina widiartinaОценок пока нет
- Main Prakriti Ebook FДокумент21 страницаMain Prakriti Ebook FddswamyОценок пока нет
- DR Cabral 7 Day Functional Liver Detox Protocol PDFДокумент20 страницDR Cabral 7 Day Functional Liver Detox Protocol PDFTyler RelphОценок пока нет
- Candida DietДокумент2 страницыCandida Dietgsekar74Оценок пока нет
- Deliverance Prayers PDFДокумент25 страницDeliverance Prayers PDFchristwitnessing75% (4)
- Memorandum PlaintiffДокумент9 страницMemorandum PlaintiffKatrina Bastareche100% (2)
- NNDrugsAidsДокумент96 страницNNDrugsAidslosangelesОценок пока нет
- PRECEDE-PROCEED Health Promotion Program Planning ModelДокумент18 страницPRECEDE-PROCEED Health Promotion Program Planning ModelLudwig GeoffreyОценок пока нет
- 10 Day Spring CleanseДокумент1 страница10 Day Spring CleanseTimОценок пока нет
- Power Over Pcos EbookДокумент160 страницPower Over Pcos EbookIra Ayu Lestari100% (2)
- Ch06 Blocked Fallopian TubesДокумент80 страницCh06 Blocked Fallopian TubesAasia Najaf SoomroОценок пока нет
- Medical Nutrition Therapy in Obesity Management - Canadian Adult Obesity Clinical Practice GuidelinesДокумент28 страницMedical Nutrition Therapy in Obesity Management - Canadian Adult Obesity Clinical Practice GuidelinesNitanluisОценок пока нет
- Shatavari - Benefits, Precautions and DosageДокумент13 страницShatavari - Benefits, Precautions and Dosagenvenkatesh485Оценок пока нет
- Blocked Fallopian TubesДокумент2 страницыBlocked Fallopian TubesPreethi JoseОценок пока нет
- Mayan Abdominal Massage For TTC-Easy Self Fertility Massage That Helped Me Get Pregnant!Документ9 страницMayan Abdominal Massage For TTC-Easy Self Fertility Massage That Helped Me Get Pregnant!miruna_macaveiОценок пока нет
- S: Alternative System of Health & Complementary Therapies: Eminar OnДокумент111 страницS: Alternative System of Health & Complementary Therapies: Eminar OnMonika shankarОценок пока нет
- DR Sara Gottfried How To Optimize Female Hormone Health For Vitality & LongevityДокумент56 страницDR Sara Gottfried How To Optimize Female Hormone Health For Vitality & Longevitywaheed khanОценок пока нет
- Ashley Sauve - Beginners Guide To Gut HealingДокумент9 страницAshley Sauve - Beginners Guide To Gut HealingChalida HayulaniОценок пока нет
- The Energetics of Health: A Naturopathic Assessment - Iva LloydДокумент4 страницыThe Energetics of Health: A Naturopathic Assessment - Iva LloydtajecygoОценок пока нет
- Thyroid Balancing Lifestyle Program - DR Katie Leah ND (February 2012)Документ8 страницThyroid Balancing Lifestyle Program - DR Katie Leah ND (February 2012)Dr Katie Leah NDОценок пока нет
- Cure For InfertilityДокумент8 страницCure For Infertilitykm_ananthОценок пока нет
- Herbal Remedies For GiardiaДокумент1 страницаHerbal Remedies For GiardiaSaad MotawéaОценок пока нет
- MaternalNutritionDietaryGuide AEDДокумент6 страницMaternalNutritionDietaryGuide AEDSandra Saenz de TejadaОценок пока нет
- Ahyanga - Ayurvedic Oil MassageДокумент2 страницыAhyanga - Ayurvedic Oil MassageSyed RahmanОценок пока нет
- Chapter 9 - Disorders Related To Menstruation PDFДокумент31 страницаChapter 9 - Disorders Related To Menstruation PDFLidia CampeanОценок пока нет
- Feeding and Eating Disorder Review LectureДокумент4 страницыFeeding and Eating Disorder Review LectureMane SharОценок пока нет
- Complete Guide to the Mayr Diet: Lose Excess Body Weight While Enjoying Your Favorite FoodsОт EverandComplete Guide to the Mayr Diet: Lose Excess Body Weight While Enjoying Your Favorite FoodsОценок пока нет
- Sample Meal PlanДокумент11 страницSample Meal PlanMihaela BrailescuОценок пока нет
- Menopause.: Becoming PregnantДокумент6 страницMenopause.: Becoming PregnantEvarista Theofika100% (1)
- Ayurveda Q&A - Detoxification Therapy Cures Fungal Infection - Sify HealthДокумент12 страницAyurveda Q&A - Detoxification Therapy Cures Fungal Infection - Sify Healthsanti_1976Оценок пока нет
- "Shankha Prakshalana" (Gastrointestinal Lavage) in Health and DiseaseДокумент8 страниц"Shankha Prakshalana" (Gastrointestinal Lavage) in Health and DiseasesoloroloОценок пока нет
- PCOS Challenge E-Zine - May 2014Документ20 страницPCOS Challenge E-Zine - May 2014PCOS Challenge, Inc.100% (1)
- Yoga Ayurveda PDF For StudentsДокумент14 страницYoga Ayurveda PDF For StudentsTijana MilenovОценок пока нет
- Fertility Diet Susan FoxДокумент35 страницFertility Diet Susan Foxnaazirah8349Оценок пока нет
- Dinacharya PDFДокумент3 страницыDinacharya PDFKrishnaswamy JajimoggalaОценок пока нет
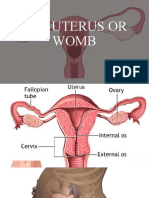
- The Uterus or WombДокумент38 страницThe Uterus or WombmuwahОценок пока нет
- Healthy Gut A Guide To Gut HealthДокумент20 страницHealthy Gut A Guide To Gut HealthKaaptan Imran khan Words0% (1)
- Ayurvedic Home RemediesДокумент3 страницыAyurvedic Home Remediesgajendra_kОценок пока нет
- One Principle For Healthy Living 19.3.12Документ129 страницOne Principle For Healthy Living 19.3.12Aman KatyalОценок пока нет
- Knowing Why We Eat, Understanding the Factors Influencing Food ChoicesОт EverandKnowing Why We Eat, Understanding the Factors Influencing Food ChoicesОценок пока нет
- Diet ManualДокумент48 страницDiet ManualBeia AcadsОценок пока нет
- Pregnancy Made Confortable With Yoga & Dietetics: Yogic exercises & nutrition to make motherhood easyОт EverandPregnancy Made Confortable With Yoga & Dietetics: Yogic exercises & nutrition to make motherhood easyОценок пока нет
- Micronutrients in PregnancyДокумент6 страницMicronutrients in Pregnancykhalisah alhadarОценок пока нет
- Health Seminar PresentationДокумент46 страницHealth Seminar Presentationmr_harshahsОценок пока нет
- Women's Hormones and Ayurveda TodayДокумент9 страницWomen's Hormones and Ayurveda TodayVishakha Saboo100% (2)
- Vitamins & Minerals ChartДокумент6 страницVitamins & Minerals ChartfarhanyazdaniОценок пока нет
- Pregnancy and YogaДокумент35 страницPregnancy and YogaPooja NadholtaОценок пока нет
- Chronic Inflammation Summit 2022 Day 3Документ5 страницChronic Inflammation Summit 2022 Day 3Paul Ioan PopescuОценок пока нет
- KSR Sweda 1Документ33 страницыKSR Sweda 1ksr prasad100% (1)
- Revelance of Shat Kriyakala in The Diagnosis and Management of Disease - .Docx by Shubham RaoДокумент6 страницRevelance of Shat Kriyakala in The Diagnosis and Management of Disease - .Docx by Shubham RaoSHUBHAM RAOОценок пока нет
- Ayurveda - VataДокумент5 страницAyurveda - VataIosef Mijkael TzadockОценок пока нет
- Panch KarmaДокумент59 страницPanch KarmavkushwahaОценок пока нет
- Uterine Fibroids: Q: What Are Fibroids? AДокумент8 страницUterine Fibroids: Q: What Are Fibroids? Abasantjain12345Оценок пока нет
- Ltyg Quick Start GuideДокумент22 страницыLtyg Quick Start Guidemarkus_naslundОценок пока нет
- Fall Cleanse GuideДокумент58 страницFall Cleanse GuideMarifé Cepeda CastroОценок пока нет
- A Guide To The Macrobiotic PrinciplesДокумент23 страницыA Guide To The Macrobiotic PrinciplesMus Oub100% (1)
- Preparing For EnemaДокумент11 страницPreparing For Enemapassion26100% (1)
- Diet InfoДокумент19 страницDiet Infoathena19Оценок пока нет
- NEW - Optimal Lab GuideДокумент22 страницыNEW - Optimal Lab GuideRamsha YasirОценок пока нет
- Maternal Care Through AyurvedaДокумент6 страницMaternal Care Through Ayurvedagaurav gupteОценок пока нет
- Relaxation and Stress Reduction for Beginners: A Mindfulness-Based ProgramОт EverandRelaxation and Stress Reduction for Beginners: A Mindfulness-Based ProgramОценок пока нет
- Sex, Sanity and Sleep!: Everything About Perimenopause and MenopauseОт EverandSex, Sanity and Sleep!: Everything About Perimenopause and MenopauseОценок пока нет
- Secret History: Kinsey's Paedophiles - Transcript ExcerptsДокумент17 страницSecret History: Kinsey's Paedophiles - Transcript ExcerptsJudith Reisman, Ph.D.100% (3)
- Sexuality Among Older Adults-Holmes sp20Документ11 страницSexuality Among Older Adults-Holmes sp20api-437977619Оценок пока нет
- Crime Topologies (Group 5)Документ48 страницCrime Topologies (Group 5)davisley28Оценок пока нет
- Malinowski Sexuallifeofsava00mali PDFДокумент746 страницMalinowski Sexuallifeofsava00mali PDFDogamDeefe100% (1)
- Gabriela Nauli C - UAS AW - 28 May 2019Документ10 страницGabriela Nauli C - UAS AW - 28 May 2019syafa nurariniОценок пока нет
- Ca Form 19-10Документ128 страницCa Form 19-10Panneer SelvamОценок пока нет
- Case Note Court: High Court of Australia Judges: Kiefel, Bell, Gageler, Keane and Nettle JJ Material FactsДокумент14 страницCase Note Court: High Court of Australia Judges: Kiefel, Bell, Gageler, Keane and Nettle JJ Material FactsSeanGong0% (1)
- 14 - Chapter 6-5 PDFДокумент56 страниц14 - Chapter 6-5 PDFsai ram100% (1)
- AbPSy 4.3Документ17 страницAbPSy 4.3히로 GuzmanОценок пока нет
- Sexology: Vladimir AntonovДокумент79 страницSexology: Vladimir AntonovFarshid RiccoОценок пока нет
- Ageing and SexualityДокумент7 страницAgeing and SexualityEsteban MatusОценок пока нет
- Influence of Parental Socio-Economic Status On The Incidence of Child Abuse and Neglect Among Primary School Pupils in Aguata Education Zone of Anambra StateДокумент83 страницыInfluence of Parental Socio-Economic Status On The Incidence of Child Abuse and Neglect Among Primary School Pupils in Aguata Education Zone of Anambra StateDebby Wura AbiodunОценок пока нет
- Sexual Homeopathic MedicineДокумент18 страницSexual Homeopathic MedicineMuhammad Rafique SeyalОценок пока нет
- 7241 Social Rehabilitation and Reintegration Notes On Sexual DeviationДокумент11 страниц7241 Social Rehabilitation and Reintegration Notes On Sexual DeviationPriscilla MumbiОценок пока нет
- Film Follies, Inc. v. Harl Haas, Etc., 426 U.S. 913 (1976)Документ3 страницыFilm Follies, Inc. v. Harl Haas, Etc., 426 U.S. 913 (1976)Scribd Government DocsОценок пока нет
- Sexually Transmitted DiseasesДокумент9 страницSexually Transmitted DiseasesRodrigo Paolo Marquina EscuadraОценок пока нет
- Human Sexual ActivityДокумент11 страницHuman Sexual ActivitynathanОценок пока нет
- Arcaba vs. BatocaelДокумент8 страницArcaba vs. BatocaelAji AmanОценок пока нет
- BBC Future TopicsДокумент120 страницBBC Future TopicsĐỗ Duy ThảoОценок пока нет
- Young Talk, August 2008Документ4 страницыYoung Talk, August 2008Straight Talk FoundationОценок пока нет
- EEOC Complainants Rebuttal To Debevoise Plimpton Report and ExhibitsДокумент44 страницыEEOC Complainants Rebuttal To Debevoise Plimpton Report and ExhibitsWXXI News100% (1)
- Sexual Fantasies and Sexual Satisfaction: An Empirical Analysis of Erotic ThoughtДокумент22 страницыSexual Fantasies and Sexual Satisfaction: An Empirical Analysis of Erotic ThoughtMădălina ŞtefaniaОценок пока нет
- Personal Development Week 1Документ23 страницыPersonal Development Week 1Sherri Bonquin100% (1)
- Nnovember Flyer OvemberДокумент12 страницNnovember Flyer OvemberGianni Di MattiaОценок пока нет
- Friday, February 10, 2012 (Sex Issue)Документ16 страницFriday, February 10, 2012 (Sex Issue)uwogazette100% (1)
- Hiv Prevalence and Associated Factors: Lawrence Marum, James N. Muttunga, Francis M. Munene, and Boaz K. ChelugetДокумент16 страницHiv Prevalence and Associated Factors: Lawrence Marum, James N. Muttunga, Francis M. Munene, and Boaz K. ChelugetHILLARY OMONDIОценок пока нет