Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- PDF Processed With Cutepdf Evaluation EditionДокумент3 страницыPDF Processed With Cutepdf Evaluation EditionShyam SunderОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Standalone Financial Results For September 30, 2016 (Result)Документ3 страницыStandalone Financial Results For September 30, 2016 (Result)Shyam SunderОценок пока нет
- Standalone Financial Results For March 31, 2016 (Result)Документ11 страницStandalone Financial Results For March 31, 2016 (Result)Shyam SunderОценок пока нет
- Standalone Financial Results, Limited Review Report For June 30, 2016 (Result)Документ3 страницыStandalone Financial Results, Limited Review Report For June 30, 2016 (Result)Shyam SunderОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Standalone Financial Results, Limited Review Report For September 30, 2016 (Result)Документ4 страницыStandalone Financial Results, Limited Review Report For September 30, 2016 (Result)Shyam SunderОценок пока нет
- Transcript of The Investors / Analysts Con Call (Company Update)Документ15 страницTranscript of The Investors / Analysts Con Call (Company Update)Shyam SunderОценок пока нет
- Investor Presentation For December 31, 2016 (Company Update)Документ27 страницInvestor Presentation For December 31, 2016 (Company Update)Shyam SunderОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Standalone Financial Results, Limited Review Report For December 31, 2016 (Result)Документ4 страницыStandalone Financial Results, Limited Review Report For December 31, 2016 (Result)Shyam SunderОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Medonic M Series Brichure PDFДокумент6 страницMedonic M Series Brichure PDFXUОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Introduction To Medtech NotesДокумент44 страницыIntroduction To Medtech NotesJanelle RemorozaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Allen Joseph Mallari Cachuela MODULE 4 NCM 114 ACT 1 AND 2Документ2 страницыAllen Joseph Mallari Cachuela MODULE 4 NCM 114 ACT 1 AND 2Marie Kelsey Acena MacaraigОценок пока нет
- 2020 List of Virtual Labs 02Документ2 страницы2020 List of Virtual Labs 02romulo182Оценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Wvgrd5c40vivpeavmmpsf3cvДокумент4 страницыWvgrd5c40vivpeavmmpsf3cvVishav Jindal100% (1)
- MyChart - Test Details PDFДокумент3 страницыMyChart - Test Details PDFAnonymous iy0yzUJOOrОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Chapter 3 - WBC Abnormalities: 3.1 NeutrophiliaДокумент25 страницChapter 3 - WBC Abnormalities: 3.1 NeutrophiliaShishir AhmedОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Philippine General HospitalДокумент5 страницPhilippine General HospitalMamski AnnОценок пока нет
- MR P SAI TEJA FINAL REPORT - LPL-1Документ4 страницыMR P SAI TEJA FINAL REPORT - LPL-1Sai GopiОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Soppi 2018Документ5 страницSoppi 2018dr_joe23Оценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
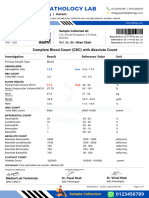
- CBC Absolute Count Test Report Format Example Sample Template Drlogy Lab ReportДокумент1 страницаCBC Absolute Count Test Report Format Example Sample Template Drlogy Lab ReportThota charanОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Presentation of The Ves-Matic Cube 30Документ4 страницыPresentation of The Ves-Matic Cube 30Tex CoОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Blood Bank Case 1 KeyДокумент4 страницыBlood Bank Case 1 KeyGissele Palero75% (8)
- Blood Chemical Test ReportДокумент1 страницаBlood Chemical Test ReportGabrielОценок пока нет
- Al-Khidmat Diagnostics Center: Department of PathologyДокумент1 страницаAl-Khidmat Diagnostics Center: Department of PathologyKiran HassanОценок пока нет
- Mythic 18Документ84 страницыMythic 18Loai AhmedОценок пока нет
- BC-5000 English Operator's Manual (7.0) PDFДокумент190 страницBC-5000 English Operator's Manual (7.0) PDFmdk25% (8)
- Medical Terminology Blood Lymph SystemsДокумент29 страницMedical Terminology Blood Lymph Systemsapi-268199514100% (1)
- Omd551/Basics of Biomedical Instrumentation Two Marks With Answer Unit I Bio Potential Generation and Electrodes TypesДокумент13 страницOmd551/Basics of Biomedical Instrumentation Two Marks With Answer Unit I Bio Potential Generation and Electrodes TypesAleesha100% (1)
- BSC MLT ResumeДокумент2 страницыBSC MLT Resumesamir_j4u50% (2)
- Assessment Hema PDFДокумент9 страницAssessment Hema PDFAnne MorenoОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Case - IUFDДокумент5 страницCase - IUFDMaris Sarline OpenianoОценок пока нет
- A B C D: MULTIPLE CHOICE - Underline The Correct AnswerДокумент5 страницA B C D: MULTIPLE CHOICE - Underline The Correct Answerエルミタ ジョイ ファティマОценок пока нет
- Erythematous Throat and Tonsils. Swollen Cervical Lymph NodesДокумент32 страницыErythematous Throat and Tonsils. Swollen Cervical Lymph NodesDr.Kuntal PatelОценок пока нет
- Neonatal Respiratory Distress SyndromeДокумент14 страницNeonatal Respiratory Distress SyndromeDrex CuritanaОценок пока нет
- Dr. Namrata .A (B.A.M.S - Mumbai)Документ23 страницыDr. Namrata .A (B.A.M.S - Mumbai)kalloornatorОценок пока нет
- 5 - 481316 - HematologyДокумент1 страница5 - 481316 - HematologyChristopher MolinaОценок пока нет
- Sysmex Xs-800i1000i Instructions For Use User's ManualДокумент210 страницSysmex Xs-800i1000i Instructions For Use User's ManualSean Chen67% (6)
- Smudge Cells:: What Technologists Need To KnowДокумент5 страницSmudge Cells:: What Technologists Need To KnowdewaОценок пока нет
- Preparation and Staining of Peripheral SmearsДокумент22 страницыPreparation and Staining of Peripheral Smearscharutha gopalОценок пока нет