Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- 108 200 1 SMДокумент6 страниц108 200 1 SMRani Oktaviani SidaurukОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- CVD Prevalence, Risk, and PathophysiologyДокумент79 страницCVD Prevalence, Risk, and PathophysiologyRani Oktaviani SidaurukОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Cholesterol Does Not Cause Heart Disease PDFДокумент20 страницCholesterol Does Not Cause Heart Disease PDFRani Oktaviani Sidauruk100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- This Month 'S Highlights: Basic Research Clinical EpidemiologyДокумент1 страницаThis Month 'S Highlights: Basic Research Clinical EpidemiologyRani Oktaviani SidaurukОценок пока нет
- Inhaled Anesthesia For BirdsДокумент18 страницInhaled Anesthesia For BirdsBianca PaludetoОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Adult Nursing 2 Math Review:Med. SurgДокумент11 страницAdult Nursing 2 Math Review:Med. Surgisapatrick8126Оценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Cynthia Stierman ResumeДокумент2 страницыCynthia Stierman Resumeapi-487498704Оценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Brochure 2019 PDFДокумент2 страницыBrochure 2019 PDFajes coolОценок пока нет
- Class IV KhodaryДокумент7 страницClass IV KhodaryelshihaweyОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Factors Influencing Permanent Teeth Eruption. Part One - General FactorsДокумент6 страницFactors Influencing Permanent Teeth Eruption. Part One - General FactorsestherОценок пока нет
- High-Dose Methotrexate, Leucovorin and Glucarpidase Dosing, Administration, and Monitoring - Adult/Pediatric - Inpatient Clinical Practice GuidelineДокумент15 страницHigh-Dose Methotrexate, Leucovorin and Glucarpidase Dosing, Administration, and Monitoring - Adult/Pediatric - Inpatient Clinical Practice GuidelineKena BenОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Oral Station Scenario PDFДокумент3 страницыOral Station Scenario PDFlotuss45Оценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Student Guide: SourceДокумент82 страницыStudent Guide: Sourcewaraney palitОценок пока нет
- Placing Piggy Back An Easy Way OutДокумент2 страницыPlacing Piggy Back An Easy Way OutMawar Putri JulicaОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Knowledge, Attitudes and Practices of The Medical Personnel Regarding Atopic Dermatitis in Yaoundé, CameroonДокумент7 страницKnowledge, Attitudes and Practices of The Medical Personnel Regarding Atopic Dermatitis in Yaoundé, CameroonNadira Juanti PratiwiОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- MDS Log BookДокумент77 страницMDS Log BookShubha Joy RakshitОценок пока нет
- Fogger, McGuinness - 2011 - Update On Energy Drinks and Youth. - Journal of Psychosocial Nursing and Mental Health ServicesДокумент3 страницыFogger, McGuinness - 2011 - Update On Energy Drinks and Youth. - Journal of Psychosocial Nursing and Mental Health ServicesOngJoonFaiiОценок пока нет
- Poison InformationДокумент27 страницPoison InformationJanvi PatelОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Surgical Endoscopy 8Документ201 страницаSurgical Endoscopy 8Saibo Boldsaikhan50% (2)
- StuffДокумент4 804 страницыStuffSonder LegariОценок пока нет
- Dialogue WritingДокумент2 страницыDialogue WritingHuma Laghari100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Syllabus Copy For PhysiotherapyДокумент108 страницSyllabus Copy For PhysiotherapyShubha DiwakarОценок пока нет
- 100 Gross Anatomy ConceptionsДокумент228 страниц100 Gross Anatomy Conceptionscrsoriano2011Оценок пока нет
- A ENT Fellowship For An Internation Resident - (Archive) - Student Doctor Network ForumsДокумент5 страницA ENT Fellowship For An Internation Resident - (Archive) - Student Doctor Network ForumsAbhishek Kumar RamadhinОценок пока нет
- INSPIRIUM BR 2Документ32 страницыINSPIRIUM BR 2Sanja PaunicОценок пока нет
- Rare Rheumatic Diseases: Springer Books Available As Printed BookДокумент1 страницаRare Rheumatic Diseases: Springer Books Available As Printed BookYUSHAОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Memory in AutismДокумент384 страницыMemory in AutismkapsicumОценок пока нет
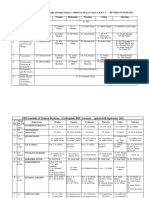
- Revised Schedule of BHU SSH OPD (Soft Copy) 2021Документ7 страницRevised Schedule of BHU SSH OPD (Soft Copy) 2021rajubhagatssmОценок пока нет
- Glasgow PhysiciansGuideДокумент90 страницGlasgow PhysiciansGuideIstván Kecskés100% (1)
- BURNS Concept MapДокумент1 страницаBURNS Concept Mapnursing concept maps100% (2)
- 2013 Different Guidelines For Imaging After First UTI in Febrile Infants - Yield, Cost and RadiationДокумент9 страниц2013 Different Guidelines For Imaging After First UTI in Febrile Infants - Yield, Cost and RadiationAnneCanapiОценок пока нет
- AnophthalmiaДокумент6 страницAnophthalmialeny zabidiОценок пока нет
- Keratoplasty 2013.en - IdДокумент8 страницKeratoplasty 2013.en - IdHanifiyah NabelaОценок пока нет
- Smile Again CaseДокумент28 страницSmile Again CaseKeshav NautiyalОценок пока нет