Вам также может понравиться
- Mechanism of Action For Each Class of AntiДокумент146 страницMechanism of Action For Each Class of AntiReynaldo RiveraОценок пока нет
- Pharmacology Drug ChartДокумент50 страницPharmacology Drug ChartEssentialForLivingОценок пока нет
- Anti HypertensivesДокумент15 страницAnti HypertensivesFaye MillanesОценок пока нет
- Drug Interactions: What Is An Interaction?Документ4 страницыDrug Interactions: What Is An Interaction?Leyla MajundaОценок пока нет
- Ultimate Pharm GuideДокумент41 страницаUltimate Pharm GuideeanguyenОценок пока нет
- Argus 5 1 Test CasesДокумент11 страницArgus 5 1 Test CasespponnapatiОценок пока нет
- KDT Only ClassificationsДокумент72 страницыKDT Only ClassificationsDebashis ParidaОценок пока нет
- (Pha) Le 5Документ19 страниц(Pha) Le 5Gabby TanОценок пока нет
- Pharmacology Notes (Chapter 20 and 21)Документ2 страницыPharmacology Notes (Chapter 20 and 21)graycorypОценок пока нет
- Whole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsДокумент17 страницWhole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsFlorina TrutescuОценок пока нет
- PCOL Maps PDFДокумент11 страницPCOL Maps PDFZinc YuloОценок пока нет
- Drug CardsДокумент3 страницыDrug CardsDave HillОценок пока нет
- DRUG SUMMARY TABLE - Anticoagulantes y AntiagregantesДокумент3 страницыDRUG SUMMARY TABLE - Anticoagulantes y AntiagregantesManuel BetancurОценок пока нет
- SNS and PNS Drugs (Cholinergics and Adrenergics)Документ5 страницSNS and PNS Drugs (Cholinergics and Adrenergics)Whitney Krabbenhoft100% (1)
- Classification of Drugs PDFДокумент15 страницClassification of Drugs PDFmuhammad ihtisham ul hassanОценок пока нет
- AntiemeticsДокумент25 страницAntiemeticsPridho GaziansyahОценок пока нет
- Review Handouts For Medical Pharmacology PDFДокумент21 страницаReview Handouts For Medical Pharmacology PDFAndres F. TorresОценок пока нет
- A New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMДокумент26 страницA New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMKartik Mendiratta100% (1)
- AntibioticsДокумент36 страницAntibioticsBen Paolo Cecilia RabaraОценок пока нет
- Pharmacology of HypertensionДокумент4 страницыPharmacology of HypertensionFlower100% (1)
- Renal Guide and Charts: AlbuminДокумент16 страницRenal Guide and Charts: AlbuminYaima JimenezОценок пока нет
- Agents Causing Coma or SeizuresДокумент3 страницыAgents Causing Coma or SeizuresShaira Aquino VerzosaОценок пока нет
- Unit III TabletsДокумент89 страницUnit III TabletsLalitha RajeshОценок пока нет
- Common Medications UsedДокумент3 страницыCommon Medications UsedRay Michael CasupananОценок пока нет
- Semester 2 Drug ListДокумент7 страницSemester 2 Drug ListNam_Pham_6481Оценок пока нет
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Документ48 страницNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanОценок пока нет
- Drug ClassДокумент13 страницDrug ClassEdfren Salazar Colon100% (1)
- Half LifeДокумент43 страницыHalf LifeMinal Nadeem100% (1)
- Pharmacology Notes: By: Khurram AbbasДокумент48 страницPharmacology Notes: By: Khurram AbbasAsma AnjumОценок пока нет
- Sem 5/unit-3 Autocoids & Related DrugsДокумент28 страницSem 5/unit-3 Autocoids & Related DrugsDARSHAN BhirudОценок пока нет
- Review Handouts For Medical Pharmacology: Terriann Crisp, PH.DДокумент28 страницReview Handouts For Medical Pharmacology: Terriann Crisp, PH.Dmus zaharaОценок пока нет
- NERVOUS MnemonicsДокумент4 страницыNERVOUS MnemonicsHimОценок пока нет
- NORADRENALINE (Norepinephrine) : Presentation DescriptionДокумент3 страницыNORADRENALINE (Norepinephrine) : Presentation DescriptionMutiaraОценок пока нет
- Pharmacology Important Things To RememberДокумент5 страницPharmacology Important Things To RememberHydie100% (1)
- Pharma MnemonicsДокумент10 страницPharma MnemonicsMuhammad Ali Aziz100% (4)
- Prefix Suffix MnemonicsДокумент5 страницPrefix Suffix MnemonicsPj MontecilloОценок пока нет
- Autacoids For Med.Документ140 страницAutacoids For Med.Feysal AhmedОценок пока нет
- Kaplan Notes. ExamenSO IMPORTANTДокумент145 страницKaplan Notes. ExamenSO IMPORTANTLisaОценок пока нет
- Adrenergic AgentsДокумент45 страницAdrenergic AgentsAmit ShahОценок пока нет
- Pharm C Exam 10 Drug ListДокумент2 страницыPharm C Exam 10 Drug ListVokdadaОценок пока нет
- ChemotherapyДокумент11 страницChemotherapyNedaAbdullahОценок пока нет
- Drugs Affecting The Autonomic Nervous System (ANS)Документ40 страницDrugs Affecting The Autonomic Nervous System (ANS)HiwaОценок пока нет
- Pharmacology A - NSAIDSДокумент14 страницPharmacology A - NSAIDSselflessdoctorОценок пока нет
- DrugsДокумент155 страницDrugsAkankshaОценок пока нет
- Pharma ChartsДокумент33 страницыPharma ChartsNooreen Hussain100% (1)
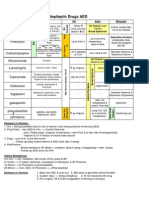
- Antiepileptic Drugs AED: D' DI Disadv SE AdvДокумент1 страницаAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Оценок пока нет
- Pall CareДокумент81 страницаPall Careडा. सत्यदेव त्यागी आर्यОценок пока нет
- Electrolytes ImbalancesДокумент4 страницыElectrolytes ImbalancesPeter John Ruiz100% (1)
- Summary of Adrenergic DrugsДокумент3 страницыSummary of Adrenergic DrugsrabduljabarrОценок пока нет
- Pharmacology Main DrugsДокумент14 страницPharmacology Main DrugsSabir KhanОценок пока нет
- Generic Name T Rade Name Classification Minitran Anti Angina NitroglycerinДокумент1 страницаGeneric Name T Rade Name Classification Minitran Anti Angina NitroglycerinChristopher LeeОценок пока нет
- Beta BlockersДокумент1 страницаBeta BlockersShrikant ThakurОценок пока нет
- Pharmacology FirecrackerДокумент37 страницPharmacology FirecrackerEinstein MKОценок пока нет
- Neuromuscular Blocking AgentsnewДокумент22 страницыNeuromuscular Blocking Agentsnewvinay0717100% (1)
- Pharm Drug ListДокумент20 страницPharm Drug Listsxymd321Оценок пока нет
- Drugs Acting On Autonomic GangliaДокумент9 страницDrugs Acting On Autonomic GangliaDita Hasni100% (1)
- PARASYMPATHOMIMETICS 201st 20yearДокумент26 страницPARASYMPATHOMIMETICS 201st 20yearFlorenz GatchalianОценок пока нет
- Study Guide PNS and CNSДокумент7 страницStudy Guide PNS and CNSsquicciariniОценок пока нет
- HAAD Exam 19 May 2016Документ13 страницHAAD Exam 19 May 2016Rehan Usman100% (3)
- Dubai Healthcare Professional Licensing Guide - Final - 2Документ141 страницаDubai Healthcare Professional Licensing Guide - Final - 2Fahad IqbalОценок пока нет
- B-No Antibiotic Prophylaxis NeededДокумент11 страницB-No Antibiotic Prophylaxis NeededRehan Usman100% (1)
- Collection of Questions From Previous HAAD ExamsДокумент34 страницыCollection of Questions From Previous HAAD ExamsRehan Usman83% (29)
- 5.Dr HishshamДокумент39 страниц5.Dr HishshamkamilbismaОценок пока нет
- Gene 3-1Документ16 страницGene 3-1Rehan UsmanОценок пока нет
- Clinical Localization and History in NeurologyДокумент41 страницаClinical Localization and History in NeurologyRhomizal MazaliОценок пока нет
- CHECKLIST Trach Care and Suctioning.Документ6 страницCHECKLIST Trach Care and Suctioning.Mickey MoraОценок пока нет
- Beltran - Diagnostic Challenges Musculoskeletal RadiologyДокумент181 страницаBeltran - Diagnostic Challenges Musculoskeletal RadiologyAndrei GianinaОценок пока нет
- MGR MPT SyllabusДокумент3 страницыMGR MPT Syllabusvictor_venki9955Оценок пока нет
- Surgical SafetyДокумент23 страницыSurgical SafetyNimi BatuboОценок пока нет
- Trigeminal NeuralgiaДокумент3 страницыTrigeminal NeuralgiaKiara PeoplesОценок пока нет
- Efficacy of Nerve Flossing Technique On Improving Sciatic Nerve Function in Patients With Sciatica - A Randomized Controlled TrialДокумент10 страницEfficacy of Nerve Flossing Technique On Improving Sciatic Nerve Function in Patients With Sciatica - A Randomized Controlled Trialsphadungkit100% (1)
- Oxygen TherapyДокумент36 страницOxygen TherapyabdihakemОценок пока нет
- Eylea FpiДокумент8 страницEylea FpiZeptii PriantiОценок пока нет
- Legal Medicine - RightsДокумент17 страницLegal Medicine - RightsRepolyo Ket Cabbage67% (3)
- Pericoronitis Is Defined As The Inflammation of The Soft Tissues of Varying Severity Around An Erupting or Partially Erupted Tooth With Breach of The FollicleДокумент7 страницPericoronitis Is Defined As The Inflammation of The Soft Tissues of Varying Severity Around An Erupting or Partially Erupted Tooth With Breach of The FollicleRavan WidiОценок пока нет
- Indian Healthcare IndustryДокумент41 страницаIndian Healthcare Industrydmathur1234Оценок пока нет
- Eye Care (Adult Critical Care)Документ19 страницEye Care (Adult Critical Care)Luffy Jemari Luffy JemariОценок пока нет
- 4.management of Vertical Discrepancies (2) 2Документ97 страниц4.management of Vertical Discrepancies (2) 2Arun Joy100% (2)
- UNIMA72 ProjectДокумент10 страницUNIMA72 ProjectJan KowalskiОценок пока нет
- A Case Presentation On:: Bipolar 1 Disorder, MRE With Psychotic FEARURESДокумент57 страницA Case Presentation On:: Bipolar 1 Disorder, MRE With Psychotic FEARURESLane Mae Magpatoc NoerrotОценок пока нет
- ENT 2014 SovedДокумент7 страницENT 2014 SovedHasnat HussainОценок пока нет
- Espondilolisis Revision 2010Документ9 страницEspondilolisis Revision 2010Giostin MosqueraОценок пока нет
- Resume 2021Документ4 страницыResume 2021api-555218722Оценок пока нет
- Kelley Eidem Recipes For CancerДокумент4 страницыKelley Eidem Recipes For CancerRohinee SinghОценок пока нет
- Tracheostomy Care Reflective EssayДокумент2 страницыTracheostomy Care Reflective EssayAnjae Gariando100% (3)
- Patient Support AreasДокумент22 страницыPatient Support AreasVivienne Rozenn LaytoОценок пока нет
- BleedingДокумент14 страницBleedingRhomizal MazaliОценок пока нет
- Chronic Myeloid Leukemia Presenting With Priapism 2329 6917 1000171Документ5 страницChronic Myeloid Leukemia Presenting With Priapism 2329 6917 1000171SalwiyadiОценок пока нет
- Suprapubic Catheter Bladder TrainingДокумент17 страницSuprapubic Catheter Bladder TrainingOrmias PratamaОценок пока нет
- Terri Campbell MAДокумент2 страницыTerri Campbell MAapi-121348673Оценок пока нет
- Aboite and About - January 2012Документ28 страницAboite and About - January 2012KPC Media Group, Inc.Оценок пока нет
- ACLS DrugДокумент7 страницACLS DrugPhongsatorn Thunin100% (1)
- Director Emergency Medical Services in Nashville TN Resume Steve FustonДокумент2 страницыDirector Emergency Medical Services in Nashville TN Resume Steve FustonSteveFustonОценок пока нет
- Insulin IssuesДокумент6 страницInsulin Issuesdoctorzo0% (1)