Вам также может понравиться
- Nursing Home Business PlanДокумент43 страницыNursing Home Business PlanSasha Dro100% (5)
- Medical Equipment and Supply Business: Your Multi Billion Dollar Guide to Start-UpОт EverandMedical Equipment and Supply Business: Your Multi Billion Dollar Guide to Start-UpОценок пока нет
- Home Care for the Elderly: Looking after Aging Loved OnesОт EverandHome Care for the Elderly: Looking after Aging Loved OnesРейтинг: 5 из 5 звезд5/5 (2)
- Nursing Home Business PlanДокумент28 страницNursing Home Business Planmineasaroeun88% (8)
- Home Health Care Services Business Plan Sample - Financial PlanДокумент11 страницHome Health Care Services Business Plan Sample - Financial Plangauravj180% (1)
- Group Home Business PlanДокумент38 страницGroup Home Business PlanDana Dang100% (13)
- Nursing Home & Assisted Living GuideДокумент73 страницыNursing Home & Assisted Living GuideYale S. HauptmanОценок пока нет
- 1034430055-Home Health Aide EnglishДокумент24 страницы1034430055-Home Health Aide EnglishHabiba KausarОценок пока нет
- Nursing Home Business PlanДокумент29 страницNursing Home Business PlanAgus Prastyo100% (1)
- Use The Nursing Home Checklist When You Visit A Nursing HomeДокумент7 страницUse The Nursing Home Checklist When You Visit A Nursing Homechapter5Оценок пока нет
- AO 2015-0052 National Policy On Palliative and Hospice Care in The PhilippinesДокумент7 страницAO 2015-0052 National Policy On Palliative and Hospice Care in The PhilippinesAldrine Albor Anyayahan I100% (1)
- Amalachukwu Maternity Home Health CareДокумент11 страницAmalachukwu Maternity Home Health CareIgbani Victory100% (1)
- Home Care Services ClarksvilleДокумент7 страницHome Care Services ClarksvilleA Caring Home Care ServicesОценок пока нет
- Assisted Living Business Plan GuidebookДокумент90 страницAssisted Living Business Plan Guidebookjohnsonkk12575% (4)
- Home Care GuideДокумент29 страницHome Care GuideNurdiansyahОценок пока нет
- Old Age Home Business PlanДокумент17 страницOld Age Home Business Planmaverickush100% (2)
- Attachment 5 - Business Plan For Skilled Nursing FacilityДокумент5 страницAttachment 5 - Business Plan For Skilled Nursing FacilityPriyesh Cheralath100% (1)
- Community and Home-Based CareДокумент86 страницCommunity and Home-Based CareBheki TshimedziОценок пока нет
- Mark E. Locklear ResumeДокумент5 страницMark E. Locklear ResumeMark LocklearОценок пока нет
- Home Care: Fatima University Medical Center FMCH DepartmentДокумент19 страницHome Care: Fatima University Medical Center FMCH DepartmentIS99057100% (1)
- Home Care Planning Guide SkilledДокумент16 страницHome Care Planning Guide SkilledswarnaОценок пока нет
- Assisted Living A Market and Technology ReviewДокумент50 страницAssisted Living A Market and Technology ReviewRehab Wahsh100% (1)
- ESAJR - Home Health Care Services - BusinessplanДокумент30 страницESAJR - Home Health Care Services - Businessplangaranzoleonievee50% (2)
- Home Health Care: Business PlanДокумент26 страницHome Health Care: Business PlanAnahit Sahakyan50% (2)
- Forms Non Medical Home Care FormsДокумент104 страницыForms Non Medical Home Care FormsAlexandru I. Din40% (5)
- Mercy Hospital Business PlanДокумент14 страницMercy Hospital Business PlanNkem Joseph-PalmerОценок пока нет
- Home Health Care Assessment ToolДокумент19 страницHome Health Care Assessment Tooljhasonify100% (2)
- Clinic Feasibility StudyДокумент20 страницClinic Feasibility StudyJeff Bergosh100% (3)
- Adult Day Care Center PDFДокумент64 страницыAdult Day Care Center PDFFlorencia Medina100% (1)
- Assisted Living Facility Consumer Fact Sheet Financial ExploitationДокумент2 страницыAssisted Living Facility Consumer Fact Sheet Financial Exploitationurbankim0% (1)
- Director of NursingДокумент3 страницыDirector of Nursingapi-78929871Оценок пока нет
- Aschiana: Afghan Children and New Approach Project ProposalДокумент6 страницAschiana: Afghan Children and New Approach Project Proposalsaher8901100% (1)
- Gena Family PlanningДокумент14 страницGena Family PlanningRuffa Jane Bangay RivasОценок пока нет
- Nursing Care at Home Business PlanДокумент4 страницыNursing Care at Home Business PlanRabindra Raj BistaОценок пока нет
- Business PlanДокумент29 страницBusiness PlanEPSONОценок пока нет
- CCCCCCCCCCCCCCCCCCCCCCC C C CCCCCCCCCCCCCCCCCCCCCCCCCC C C C C C CДокумент6 страницCCCCCCCCCCCCCCCCCCCCCCC C C CCCCCCCCCCCCCCCCCCCCCCCCCC C C C C C CArbaaz Kazi100% (1)
- Guidebook On Nursing HomesДокумент55 страницGuidebook On Nursing HomestruefireОценок пока нет
- Home Health Agencies, Chapter 111-8-31Документ20 страницHome Health Agencies, Chapter 111-8-31Tyria GoinesОценок пока нет
- Hospital ProposalДокумент5 страницHospital ProposalSushant Sharma100% (1)
- Homecare LTD 1Документ61 страницаHomecare LTD 1m0k123_112640140Оценок пока нет
- 10 Things Your Assisted-Living Facility Won't Tell You - SmartMoney PDFДокумент8 страниц10 Things Your Assisted-Living Facility Won't Tell You - SmartMoney PDFPraful RathoreОценок пока нет
- How To Write A Assisted Living Facility Business PlanДокумент20 страницHow To Write A Assisted Living Facility Business PlanKhun Walter100% (2)
- Nursing Home Business PlanДокумент27 страницNursing Home Business PlanKeanuОценок пока нет
- Nursing Home Lesson PlanДокумент13 страницNursing Home Lesson Planapi-353466401100% (1)
- The Hospital Case ManagementДокумент39 страницThe Hospital Case ManagementRirien Triana Suhaeli80% (5)
- 100 Beded Cancer HospitalДокумент23 страницы100 Beded Cancer Hospitalsureshvgk100% (1)
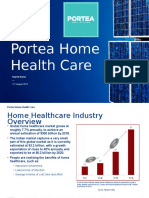
- Portea Home Health CareДокумент17 страницPortea Home Health CareAbhai Pratap SinghОценок пока нет
- Business Plan-Staffing AgencyДокумент8 страницBusiness Plan-Staffing AgencyRichard Chiu67% (3)
- H C I M U: Ealth ARE Ndustry Arket PdateДокумент24 страницыH C I M U: Ealth ARE Ndustry Arket PdateRavi RanjanОценок пока нет
- Implementation Plan For Addus HomeCareДокумент9 страницImplementation Plan For Addus HomeCaredbear0% (1)
- Medical Laboratory Business Plan For Starting Your Own Research CenterДокумент50 страницMedical Laboratory Business Plan For Starting Your Own Research CenterIqbal Burcha ConsultantОценок пока нет
- Business Plan Medical ClinicДокумент47 страницBusiness Plan Medical ClinicHassan Omar100% (3)
- Client HandbookДокумент20 страницClient HandbookTheresia Lumban Gaol80% (5)
- Business Proposal For Heartland HealthДокумент20 страницBusiness Proposal For Heartland Healthapi-3942622340% (1)
- El1 - Palliative & Hospice Care in The PhilippinesДокумент49 страницEl1 - Palliative & Hospice Care in The PhilippinesStudentnurseMj50% (4)
- Rural MEdical Camps - PDF FinalДокумент32 страницыRural MEdical Camps - PDF FinalKashish KhuranaОценок пока нет
- A Guide To Getting Started in TelemedicineДокумент405 страницA Guide To Getting Started in TelemedicineAnthony WilsonОценок пока нет
- Aging PDFДокумент24 страницыAging PDFNeha JayaramanОценок пока нет
- Nursing Care Plan: Assessment DataДокумент2 страницыNursing Care Plan: Assessment DataDana CozorocОценок пока нет
- Restraint ProtocolДокумент4 страницыRestraint ProtocolsrinivasanaОценок пока нет
- 200 Bed Hospital Project ReportДокумент40 страниц200 Bed Hospital Project Reportsaleha sultanaОценок пока нет
- How To Start An Adult Day Care Center in TexasДокумент5 страницHow To Start An Adult Day Care Center in TexascoopernicuzОценок пока нет
- Karnataka Private Nursing Homes (Regulation) Act, 1976Документ6 страницKarnataka Private Nursing Homes (Regulation) Act, 1976Latest Laws TeamОценок пока нет
- Long Term LivingДокумент168 страницLong Term LivingJohann Victorious-Redd SmithОценок пока нет
- Bhs 2007 Minimum Design Standards Final PDF Doc. 198958 7Документ149 страницBhs 2007 Minimum Design Standards Final PDF Doc. 198958 7eng_tulipe100% (1)
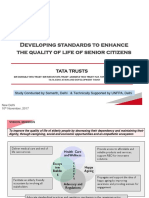
- Tata Trusts - Samarth Presentation - 091117Документ29 страницTata Trusts - Samarth Presentation - 091117varma1234Оценок пока нет
- Family Medicare Policy-ProspectusДокумент11 страницFamily Medicare Policy-ProspectusRKОценок пока нет
- Nutrition Lesson 11 K RD411 Resident Rights InserviceДокумент3 страницыNutrition Lesson 11 K RD411 Resident Rights InserviceMashaal FasihОценок пока нет
- California Code of RegulationsДокумент19 страницCalifornia Code of RegulationsAMEU URGENCIASОценок пока нет
- Ninjas Finding Missing Covid-19 Contact Links: 24 Contacts To Hunt Per Positive PatientДокумент44 страницыNinjas Finding Missing Covid-19 Contact Links: 24 Contacts To Hunt Per Positive Patientluvnuts4u luvnutsОценок пока нет
- 9 6 Policy On Quality Assurance in Health Care ServicesДокумент7 страниц9 6 Policy On Quality Assurance in Health Care ServicesSujan AcharyaОценок пока нет
- Mackemull Vs Brian Center PDFДокумент26 страницMackemull Vs Brian Center PDFDenise PridgenОценок пока нет
- Discipline and Ideas Module 3Документ43 страницыDiscipline and Ideas Module 3Manelyn Taga75% (8)
- Documentation Template For Physical Therapist Patient/Client ManagementДокумент6 страницDocumentation Template For Physical Therapist Patient/Client ManagementRaquel VBОценок пока нет
- The PortfolioДокумент39 страницThe Portfolioapi-284740045100% (1)
- EditionДокумент28 страницEditionSan Mateo Daily JournalОценок пока нет
- VA Complete RegsДокумент47 страницVA Complete RegsTJSОценок пока нет
- Access Letter Requesting Permission To Conduct Research 4Документ7 страницAccess Letter Requesting Permission To Conduct Research 4Angelica Mercado SirotОценок пока нет
- 10th BPS - JOINT NOTE 2015 PDFДокумент49 страниц10th BPS - JOINT NOTE 2015 PDFAnjaiah MandeОценок пока нет
- FL Medicaid Managed Care FAQДокумент85 страницFL Medicaid Managed Care FAQJenniferRaePittsОценок пока нет
- Critical Care Nursing CNA 2007Документ93 страницыCritical Care Nursing CNA 2007Netinh3Оценок пока нет
- Wake County Stay-At-Home OrderДокумент11 страницWake County Stay-At-Home OrderDavid PurtellОценок пока нет
- Happy Family Floater Prospectus 06052015Документ16 страницHappy Family Floater Prospectus 06052015Soumen PaulОценок пока нет
- Health Assessment FormДокумент8 страницHealth Assessment FormIrina Chpitalnik100% (1)
- 2011 Montreal Conference Abstract BookДокумент0 страниц2011 Montreal Conference Abstract BookNona Delia Chiriac100% (1)
- GIPSAДокумент37 страницGIPSAsohalsingh1Оценок пока нет
- Health Care Information Management For Senior Citizen Capstone DocumentationДокумент7 страницHealth Care Information Management For Senior Citizen Capstone DocumentationYvonn NisperosОценок пока нет