Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Essential Neurology 4Th Ed PDFДокумент290 страницEssential Neurology 4Th Ed PDFPutu 'yayuk' Widyani WiradiraniОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- HL Biology IA 20/24Документ14 страницHL Biology IA 20/24dev0% (1)
- Bab 358 Regurgitasi Mitral PDFДокумент5 страницBab 358 Regurgitasi Mitral PDFMuhammad IhsanuddinОценок пока нет
- Presentation Illustrating The 2017 Classification of Seizure TypesДокумент54 страницыPresentation Illustrating The 2017 Classification of Seizure TypesMohamad Syaikhul IslamОценок пока нет
- Bab 125 Glomerulonefritis PDFДокумент4 страницыBab 125 Glomerulonefritis PDFMuhammad IhsanuddinОценок пока нет
- Bab 339 Pemeriksaan Kardiologi Nuklir PDFДокумент2 страницыBab 339 Pemeriksaan Kardiologi Nuklir PDFMuhammad IhsanuddinОценок пока нет
- Path o Physiology ConciousnessДокумент4 страницыPath o Physiology ConciousnessaristadevyaОценок пока нет
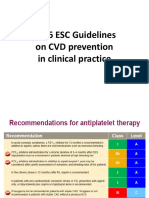
- 2016 ESC Guidelines On CVD Prevention in Clinical PracticeДокумент8 страниц2016 ESC Guidelines On CVD Prevention in Clinical PracticeMuhammad IhsanuddinОценок пока нет
- Mechanism Molecular SepsisДокумент4 страницыMechanism Molecular SepsisMuhammad IhsanuddinОценок пока нет
- Bab 334 Radiologi Jantung PDFДокумент4 страницыBab 334 Radiologi Jantung PDFMuhammad IhsanuddinОценок пока нет
- Referat Airway ManagementДокумент24 страницыReferat Airway ManagementVerarisnaОценок пока нет
- Ringkasan Dosis Obat 7th RevisedДокумент38 страницRingkasan Dosis Obat 7th RevisedMuhammad IhsanuddinОценок пока нет
- Dry Eye Syndrome PPPДокумент44 страницыDry Eye Syndrome PPPHendra GunawanОценок пока нет
- Referat Airway ManagementДокумент24 страницыReferat Airway ManagementVerarisnaОценок пока нет
- 2 Airway ManagementДокумент15 страниц2 Airway ManagementEinz Nur Amalyah IdrusОценок пока нет
- Ipa Belum Di TranslateДокумент5 страницIpa Belum Di TranslateMuhammad IhsanuddinОценок пока нет
- Mechanism Molecular SepsisДокумент4 страницыMechanism Molecular SepsisMuhammad IhsanuddinОценок пока нет
- Handayani RahmaДокумент6 страницHandayani RahmaMuhammad IhsanuddinОценок пока нет
- UTI Treatment Guidelines PDFДокумент5 страницUTI Treatment Guidelines PDFMuhammad IhsanuddinОценок пока нет
- BIEN DKKДокумент15 страницBIEN DKKMuhammad IhsanuddinОценок пока нет
- WHO - Diarrhoeal DiseaseДокумент4 страницыWHO - Diarrhoeal DiseaseMuhammad IhsanuddinОценок пока нет
- Examination of The Eye - GitaДокумент71 страницаExamination of The Eye - GitaMuhammad IhsanuddinОценок пока нет
- Cardiac Muscle Refractory PeriodДокумент7 страницCardiac Muscle Refractory PeriodEngku FaisalОценок пока нет
- Daftar PTCДокумент1 страницаDaftar PTCMuhammad IhsanuddinОценок пока нет
- Secondary Immunodeficiency in ChildrenДокумент16 страницSecondary Immunodeficiency in Childrenryan20eОценок пока нет
- SGS Daily Light Integral Research StudyДокумент10 страницSGS Daily Light Integral Research Studyhari HaranОценок пока нет
- American Journal of Agricultural EconomicsДокумент3 страницыAmerican Journal of Agricultural EconomicsRey DoankОценок пока нет
- Physical Agents Used in The Management of Chronic Pain by Physical TherapistsДокумент31 страницаPhysical Agents Used in The Management of Chronic Pain by Physical TherapistsMárcia MatosОценок пока нет
- Snakes of The World A Supplement by Boundy Jeff WallachДокумент284 страницыSnakes of The World A Supplement by Boundy Jeff WallachRoullienОценок пока нет
- Syndactyly 1Документ13 страницSyndactyly 1AminullahОценок пока нет
- Manchester Ship Canal - Strategic Review of Fish PopulationsДокумент139 страницManchester Ship Canal - Strategic Review of Fish PopulationsSamyuktha PillaiОценок пока нет
- Beckman ProtocolДокумент34 страницыBeckman ProtocolIonut NeagaОценок пока нет
- 3 5 18 950 PDFДокумент3 страницы3 5 18 950 PDFBang AthanОценок пока нет
- Chemistry I TheoryДокумент2 страницыChemistry I Theory17roopa2010Оценок пока нет
- QC ABO RH BloodДокумент62 страницыQC ABO RH BloodrhoderickОценок пока нет
- P. 134-149Документ16 страницP. 134-149biblioagroОценок пока нет
- Combined Stresses in PlantsДокумент281 страницаCombined Stresses in Plantsmdg21Оценок пока нет
- Lionex LIOFeronTB LTBIДокумент2 страницыLionex LIOFeronTB LTBIBilgi KurumsalОценок пока нет
- SMA GAMA YOGYAKARTA English PAT FormДокумент12 страницSMA GAMA YOGYAKARTA English PAT FormVivit Pramita100% (1)
- 21 Day Brain DetoxДокумент16 страниц21 Day Brain DetoxJoycechan87100% (1)
- The Study of Life: Teacher Notes and AnswersДокумент4 страницыThe Study of Life: Teacher Notes and AnswersHector AguilarОценок пока нет
- Formulation and Evaluation of Moxifloxacin Loaded Alginate Chitosan NanoparticlesДокумент5 страницFormulation and Evaluation of Moxifloxacin Loaded Alginate Chitosan NanoparticlesSriram NagarajanОценок пока нет
- Kung Et Al. (2018)Документ14 страницKung Et Al. (2018)Henry Daniel Ruiz AlbaОценок пока нет
- Lauryl Tryptose Broth - LiofilchemДокумент4 страницыLauryl Tryptose Broth - LiofilchemMitha AriantiОценок пока нет
- Etiologji Dhe Epidemiologjia e StrokeДокумент7 страницEtiologji Dhe Epidemiologjia e StrokegranitОценок пока нет
- Healthy Weekly Meal Plan Highlights Biomolecule NutritionДокумент4 страницыHealthy Weekly Meal Plan Highlights Biomolecule NutritionAndrie DatulОценок пока нет
- Genetic Algorithm Based PID Control Tuning For A Model BioreactorДокумент13 страницGenetic Algorithm Based PID Control Tuning For A Model BioreactorertyucbОценок пока нет
- (Methods in Molecular Medicine) S. Moira Brown, Alasdair R. MacLean - Herpes Simplex Virus Protocols (1998, Humana Press)Документ406 страниц(Methods in Molecular Medicine) S. Moira Brown, Alasdair R. MacLean - Herpes Simplex Virus Protocols (1998, Humana Press)Rares TautОценок пока нет
- Cadmium Tolerance in Schinus Molle Trees Is Modulated by Enhanced Leaf Anatomy and PhotosynthesisДокумент8 страницCadmium Tolerance in Schinus Molle Trees Is Modulated by Enhanced Leaf Anatomy and PhotosynthesisPaulinho TemoteoОценок пока нет
- Activity 5 Type of Root SystemДокумент2 страницыActivity 5 Type of Root SystemPreiy Julian De GuiaОценок пока нет
- Hurdle TechnologyДокумент5 страницHurdle TechnologyDavid UribeОценок пока нет
- B0 29palms 01 31 2017Документ148 страницB0 29palms 01 31 2017The Press-Enterprise / pressenterprise.comОценок пока нет
- 2013 Taruka Mammalian SpeciesДокумент12 страниц2013 Taruka Mammalian SpeciesabrunomirandacОценок пока нет