Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Combination Treatment of Benzodiazepine and SsriДокумент7 страницCombination Treatment of Benzodiazepine and SsriNararto PrijogoОценок пока нет
- Metformin and Reduced Risk of Hepatocellular Carcinoma in Diabetes With CLDДокумент9 страницMetformin and Reduced Risk of Hepatocellular Carcinoma in Diabetes With CLDNararto PrijogoОценок пока нет
- Aminotransferase Elevations in Healthy Adults Receiving 4 Grams of Acetaminophen DailyДокумент7 страницAminotransferase Elevations in Healthy Adults Receiving 4 Grams of Acetaminophen DailyNararto PrijogoОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- VasДокумент4 страницыVasRaluca RaluОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- VasДокумент4 страницыVasRaluca RaluОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Faces Pain Scale PDFДокумент4 страницыFaces Pain Scale PDFNararto PrijogoОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Preprandial and Post Prandial - Wanita HamilДокумент5 страницPreprandial and Post Prandial - Wanita HamilNararto PrijogoОценок пока нет
- A Clinical Guide To Using IV PPI in Reflux and Peptic UlcersДокумент12 страницA Clinical Guide To Using IV PPI in Reflux and Peptic UlcersNararto PrijogoОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Combination Treatment of Benzodiazepine and SsriДокумент7 страницCombination Treatment of Benzodiazepine and SsriNararto PrijogoОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Depression in Adults Recognition and Management NICE 2009 PDFДокумент64 страницыDepression in Adults Recognition and Management NICE 2009 PDFNararto PrijogoОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Systematic Review Direct Comparative Trials of The Efficacy of PPIДокумент10 страницSystematic Review Direct Comparative Trials of The Efficacy of PPINararto PrijogoОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Paracetamol Use Dec 2008Документ30 страницParacetamol Use Dec 2008Nararto PrijogoОценок пока нет
- Depression in Adults Recognition and Management NICE 2009 PDFДокумент64 страницыDepression in Adults Recognition and Management NICE 2009 PDFNararto PrijogoОценок пока нет
- Comparison Effect Metformin Glimepiride and Metformin Glibenclamide in PX DM2Документ12 страницComparison Effect Metformin Glimepiride and Metformin Glibenclamide in PX DM2Nararto PrijogoОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Elevated Liver Enzymes in Patients With CholecystitisДокумент4 страницыElevated Liver Enzymes in Patients With CholecystitisMuhammad Syamil RozlanОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- DM Before and After OperateДокумент5 страницDM Before and After OperateNararto PrijogoОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Preprandial and Post Prandial - Wanita HamilДокумент5 страницPreprandial and Post Prandial - Wanita HamilNararto PrijogoОценок пока нет
- CLN 67 11 1259Документ5 страницCLN 67 11 1259Nararto PrijogoОценок пока нет
- Evaluation of A Protocol For The Non-OperatifДокумент4 страницыEvaluation of A Protocol For The Non-OperatifNararto PrijogoОценок пока нет
- Manajemen Sepsis - SSCДокумент8 страницManajemen Sepsis - SSCDeborah Bravian TairasОценок пока нет
- Zac 1315Документ5 страницZac 1315Nararto PrijogoОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Gallstones and Choledocolithiasis With Severe Cholestatic Jaundice inДокумент5 страницGallstones and Choledocolithiasis With Severe Cholestatic Jaundice inNararto PrijogoОценок пока нет
- AДокумент4 страницыANararto PrijogoОценок пока нет
- DM Before and After OperateДокумент5 страницDM Before and After OperateNararto PrijogoОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- American Journal of Epidemiology Volume 167 Issue 12 2008 (Doi 10.1093/aje/kwn075) Leung, C. C. Lam, T. H. Chan, W. M. Yew, W. W. Ho, K. S. Le - Diabetic Control and Risk of Tuberculosis - A PDFДокумент9 страницAmerican Journal of Epidemiology Volume 167 Issue 12 2008 (Doi 10.1093/aje/kwn075) Leung, C. C. Lam, T. H. Chan, W. M. Yew, W. W. Ho, K. S. Le - Diabetic Control and Risk of Tuberculosis - A PDFNararto PrijogoОценок пока нет
- Bronchodilator Beta2 AgonistДокумент3 страницыBronchodilator Beta2 AgonistNararto PrijogoОценок пока нет
- My Lan FentanylДокумент5 страницMy Lan FentanylNararto PrijogoОценок пока нет
- IV Fluid ManagementДокумент10 страницIV Fluid ManagementNararto PrijogoОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Alt Ast Alp GGT Pada Liver DiseaseДокумент5 страницAlt Ast Alp GGT Pada Liver DiseaseNararto PrijogoОценок пока нет
- First Malaria VaccineДокумент3 страницыFirst Malaria VaccineNararto PrijogoОценок пока нет
- Chapter 37: Drugs Used To Treat Thyroid DiseaseДокумент40 страницChapter 37: Drugs Used To Treat Thyroid DiseaseAziil LiizaОценок пока нет
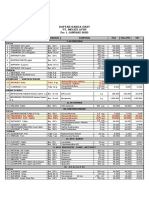
- Daftar Harga Obat - Pt. Molex Ayus - Januari 2023Документ4 страницыDaftar Harga Obat - Pt. Molex Ayus - Januari 2023Muhammad AdninОценок пока нет
- Drug StudyДокумент6 страницDrug StudychaОценок пока нет
- Rational Use of SteroidsДокумент15 страницRational Use of SteroidsPrayoga SiraitОценок пока нет
- Disorders of The Adrenal GlandsДокумент9 страницDisorders of The Adrenal Glandsmoon businessОценок пока нет
- An Assignment On Routinely Use Drugs in Our Clinic: Submitted To: Submitted byДокумент48 страницAn Assignment On Routinely Use Drugs in Our Clinic: Submitted To: Submitted byIbad Ur Rahman100% (1)
- Þ" Hospital: Clinical and Scientific Rationale For The "MATH Treatment Protocol For COVID-19Документ22 страницыÞ" Hospital: Clinical and Scientific Rationale For The "MATH Treatment Protocol For COVID-19Doménica SánchezОценок пока нет
- Uso de Esteroides en AnestesiaДокумент7 страницUso de Esteroides en AnestesiatitinodeОценок пока нет
- Methylprednisolone (Solu Medrol)Документ3 страницыMethylprednisolone (Solu Medrol)Adrianne Bazo100% (1)
- Role of Steroids in Critical Care PDFДокумент3 страницыRole of Steroids in Critical Care PDFDr.Shilpa JohnОценок пока нет
- FLCCC Protocols - A Guide To The Management of COVID 19Документ61 страницаFLCCC Protocols - A Guide To The Management of COVID 19Tina SangreaОценок пока нет
- Pharma - SkinДокумент8 страницPharma - Skinreference books100% (1)
- Practice ComputationДокумент5 страницPractice Computationnictan 14Оценок пока нет
- Drug Study MethylprednisoloneДокумент4 страницыDrug Study MethylprednisolonePao LaurenteОценок пока нет
- 50 Item Practice ExamДокумент8 страниц50 Item Practice ExamHasan A AsFourОценок пока нет
- Eular SLE 2023Документ15 страницEular SLE 2023DeddyОценок пока нет
- Memorial For The ComplainantДокумент32 страницыMemorial For The ComplainantArpit BansalОценок пока нет
- Massachusetts General Hospital (MGH) COVID-19 Treatment GuidanceДокумент24 страницыMassachusetts General Hospital (MGH) COVID-19 Treatment Guidancerajesh BОценок пока нет
- CC Junsay Nicole Xyza T. Learning Interaction FormДокумент10 страницCC Junsay Nicole Xyza T. Learning Interaction FormNicole Xyza JunsayОценок пока нет
- Lupus: PrintДокумент24 страницыLupus: Printmelodia gandezaОценок пока нет
- The Side Effects of Corticosteroids: Bernard BeckerДокумент6 страницThe Side Effects of Corticosteroids: Bernard BeckerShayyy JacksonОценок пока нет
- A Case Study Oftraumatic Spinal Cord InjuryДокумент111 страницA Case Study Oftraumatic Spinal Cord InjuryJUDE ARIZALA100% (1)
- MOH Therapeutic Protocol For COVID 19Документ12 страницMOH Therapeutic Protocol For COVID 19Faris Thomas FarisОценок пока нет
- Drug StudyДокумент4 страницыDrug Studyw dОценок пока нет
- Pre Op GuidelinesДокумент11 страницPre Op GuidelinesHanif FebrianОценок пока нет
- Acute Exacerbation of AsthmaДокумент31 страницаAcute Exacerbation of AsthmaMuneeb YounisОценок пока нет
- Soal Acak Orthobullets 2019Документ131 страницаSoal Acak Orthobullets 2019kristinaОценок пока нет
- Steroids in Chronic Subdural Hematomas SUCRE TrialДокумент8 страницSteroids in Chronic Subdural Hematomas SUCRE TrialEdward Arthur IskandarОценок пока нет
- Exam Cram CardДокумент2 страницыExam Cram CardVietnam Vo100% (1)
- 22PG MATH-plus-Rationale-Journal-of-Intensive-Care-Medicine-Dec2020Документ22 страницы22PG MATH-plus-Rationale-Journal-of-Intensive-Care-Medicine-Dec2020Barbara RoweОценок пока нет
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (80)