Вам также может понравиться
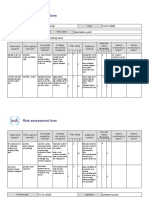
- Risk Assessment Project Iosh - MsДокумент2 страницыRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- Pharmacology Practice Test IДокумент27 страницPharmacology Practice Test Isidharta_chatterjeeОценок пока нет
- Acute Ischemic Stroke: by Steven H. Nakajima, Pharm.D., BCCCP and Katleen Wyatt Chester, Pharm.D., BCCCP, BCGPДокумент26 страницAcute Ischemic Stroke: by Steven H. Nakajima, Pharm.D., BCCCP and Katleen Wyatt Chester, Pharm.D., BCCCP, BCGPCristian Florin CrasmaruОценок пока нет
- Chronic Kidney DiseaseДокумент40 страницChronic Kidney DiseasePaul SinsОценок пока нет
- VK-53 (ВК-53) Erecting Cut-Out Switch: Maintenance ManualДокумент76 страницVK-53 (ВК-53) Erecting Cut-Out Switch: Maintenance ManualhaileОценок пока нет
- 6.m.tech-Ece-Vlsi, Vlsi Systems, Vlsi System Design (Vlsi, Vlsis, Vlsisd) r17 Course Structure & SyllabiДокумент35 страниц6.m.tech-Ece-Vlsi, Vlsi Systems, Vlsi System Design (Vlsi, Vlsis, Vlsisd) r17 Course Structure & SyllabiravibabukancharlaОценок пока нет
- Ace of Spades + Outlaw 125 2019Документ85 страницAce of Spades + Outlaw 125 2019Nelson RodrigoОценок пока нет
- Drugs For HyperlipidemiaДокумент29 страницDrugs For Hyperlipidemiasultan khabeebОценок пока нет
- Hyperlipidemia: Revised: October 4, 2019Документ7 страницHyperlipidemia: Revised: October 4, 2019HannaОценок пока нет
- CVS MCQS 06 QДокумент2 страницыCVS MCQS 06 Qharshad patelОценок пока нет
- COPD ExacerbationДокумент2 страницыCOPD ExacerbationjusthoangОценок пока нет
- LiverTox: Clinical and Research Information On Drug-Induced Liver Injury - AcetaminophenДокумент41 страницаLiverTox: Clinical and Research Information On Drug-Induced Liver Injury - AcetaminophenJessica AristaОценок пока нет
- Clinical Pharmacy Lab - Quiz Part 2Документ4 страницыClinical Pharmacy Lab - Quiz Part 2Aassh DcmbrОценок пока нет
- AutacoidsДокумент32 страницыAutacoidsRenellie TrimidalОценок пока нет
- Cagayan State University College of Medicine and Surgery SY: 2009-2010Документ41 страницаCagayan State University College of Medicine and Surgery SY: 2009-2010ahmad usmanОценок пока нет
- Chemical Pathology II HIV AIDSДокумент33 страницыChemical Pathology II HIV AIDSSimeon AdebisiОценок пока нет
- Antiplatelet, Anticoagulant and Thrombolytic Agents: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213Документ30 страницAntiplatelet, Anticoagulant and Thrombolytic Agents: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213JedoОценок пока нет
- 1 Drugs Affecting The Endocrine SystemДокумент61 страница1 Drugs Affecting The Endocrine SystemHERLIN HOBAYANОценок пока нет
- Electrolyte Replacement Guide - ICU CliniciansДокумент8 страницElectrolyte Replacement Guide - ICU Cliniciansnolan4266Оценок пока нет
- Anemia Prevention and Management Program Implementation GuideДокумент60 страницAnemia Prevention and Management Program Implementation GuideIchlasul MadriddistaОценок пока нет
- Alawlaqi - Obesity FinalДокумент26 страницAlawlaqi - Obesity FinalMotea Alawlaqi100% (1)
- 8B - Antianginal DrugsДокумент70 страниц8B - Antianginal Drugslalitrajindolia100% (1)
- P7b11toc Gastroenterology and NutritionДокумент19 страницP7b11toc Gastroenterology and NutritionWidya Lestari CapawatyОценок пока нет
- Final Test Modul 1-2 Medicine New BaseДокумент102 страницыFinal Test Modul 1-2 Medicine New BasePurnima ChoudhuryОценок пока нет
- 1 ❤ Smart Sheet for History Taking in Internal Medicine خلفية سماويةДокумент12 страниц1 ❤ Smart Sheet for History Taking in Internal Medicine خلفية سماويةOsama A100% (1)
- Drug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineДокумент21 страницаDrug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineAtakan Yeşil100% (1)
- Lipid Metabolism - WikipediaДокумент31 страницаLipid Metabolism - WikipediaTomiwa AdeshinaОценок пока нет
- Pharmacotherapy of Heart Failure: Abera J. (Bpharm., MSC in Clinical Pharmacy) School of Pharmacy, CHMS, HuДокумент79 страницPharmacotherapy of Heart Failure: Abera J. (Bpharm., MSC in Clinical Pharmacy) School of Pharmacy, CHMS, HuAbera JamboОценок пока нет
- Beta BlockersДокумент70 страницBeta BlockersIrina Cabac-PogoreviciОценок пока нет
- Decision Algorithm For Prescribing SGLT2 Inhibitors and GLP-1 Receptor AgonistsДокумент11 страницDecision Algorithm For Prescribing SGLT2 Inhibitors and GLP-1 Receptor AgonistsNati BocciaОценок пока нет
- Workbook 2016 StomДокумент186 страницWorkbook 2016 StomAysenОценок пока нет
- Pharmacology Question Bank BPTДокумент5 страницPharmacology Question Bank BPTJoHN SamueLОценок пока нет
- MCQS ANS 02 SolДокумент5 страницMCQS ANS 02 SolSamir Rekha Mukund Joshi100% (1)
- Goodman and Gilman39s Manual of Pharmacology and Therapeutics Latest EditionДокумент3 страницыGoodman and Gilman39s Manual of Pharmacology and Therapeutics Latest EditionLinda0% (1)
- NORADRENALINE (Norepinephrine) : Presentation DescriptionДокумент3 страницыNORADRENALINE (Norepinephrine) : Presentation DescriptionMutiaraОценок пока нет
- Inborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Документ4 страницыInborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Wen Jie LauОценок пока нет
- Nsaids 190204194047Документ40 страницNsaids 190204194047Harini Bala100% (1)
- Management of Diabetes MellitusДокумент42 страницыManagement of Diabetes Mellitusayu ersa lestari100% (1)
- Pharmacology Terms & DefinitionДокумент10 страницPharmacology Terms & DefinitionKabirОценок пока нет
- MCQДокумент17 страницMCQpradeephdОценок пока нет
- Metabolism of LipidsДокумент47 страницMetabolism of LipidsMarwahОценок пока нет
- Exercise 9 - Renal System PhysiologyДокумент18 страницExercise 9 - Renal System Physiologynhungto740% (1)
- Pharmacy PracticeДокумент17 страницPharmacy PracticeP D SpencerОценок пока нет
- DyslipidemiaДокумент18 страницDyslipidemiaDeepthi Avvaru100% (1)
- Pharmacotherapy of DMДокумент23 страницыPharmacotherapy of DMsalinaОценок пока нет
- Ch-13 Drugs Used in Heart FailureДокумент49 страницCh-13 Drugs Used in Heart FailureShabrin SadikhОценок пока нет
- Pre Assessment Diabetes Nursing CareДокумент4 страницыPre Assessment Diabetes Nursing CareHabib UllahОценок пока нет
- Pathphys ModuleДокумент102 страницыPathphys ModuleRodriguez Vivanco Kevin DanielОценок пока нет
- Guidline EndocarditisДокумент54 страницыGuidline EndocarditisIrfan MohammadОценок пока нет
- 14 NSAIDS LastДокумент46 страниц14 NSAIDS LastMewael TesfamichaelОценок пока нет
- Name Honor Pledge (Signature) : Questions 1 - 2 Refer To The Following CaseДокумент9 страницName Honor Pledge (Signature) : Questions 1 - 2 Refer To The Following CasegregstevensОценок пока нет
- 4 2 KdigoДокумент242 страницы4 2 KdigoPatricia Denise Tome MagisaОценок пока нет
- Anticholinergic DrugsДокумент19 страницAnticholinergic DrugseashshankarОценок пока нет
- Chap253-Heart Failure ManagementДокумент42 страницыChap253-Heart Failure ManagementDoctor CastleОценок пока нет
- ACE 2007 4A QuestionsДокумент29 страницACE 2007 4A QuestionsRachana GudipudiОценок пока нет
- AclsДокумент2 страницыAclsEman ElzeftawyОценок пока нет
- CNS DepressantsДокумент69 страницCNS DepressantsMicah Lou Calamba100% (1)
- Complement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtДокумент70 страницComplement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtCherry Reyes-Principe100% (1)
- Autonomic Nervous System YASER BIDAHДокумент19 страницAutonomic Nervous System YASER BIDAHGhalia Tarek Al Hassan100% (2)
- Liver Cirrhosis: DR Alex MogereДокумент51 страницаLiver Cirrhosis: DR Alex MogereGladys Maina100% (1)
- 6-8 Thrombolitics Antiplatelet AnticoagulantДокумент36 страниц6-8 Thrombolitics Antiplatelet AnticoagulantFatima ZahraОценок пока нет
- EnglishДокумент56 страницEnglishPankaj SharmaОценок пока нет
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingОт EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováОценок пока нет
- Clinical Physiology and Pharmacology: The EssentialsОт EverandClinical Physiology and Pharmacology: The EssentialsРейтинг: 4 из 5 звезд4/5 (1)
- r315 Quick Start PDFДокумент80 страницr315 Quick Start PDFfdsfasdsfadsОценок пока нет
- Maxon - Gas Electro-Mechanical ValvesДокумент4 страницыMaxon - Gas Electro-Mechanical ValvesThiagoОценок пока нет
- Agriculture Mcqs PDFДокумент4 страницыAgriculture Mcqs PDFAbdul QudoosОценок пока нет
- What Is Geyi - V MairДокумент31 страницаWhat Is Geyi - V MairbodhitanОценок пока нет
- Mechanical Components SectionДокумент428 страницMechanical Components Sectionxristo xristovОценок пока нет
- Ncs University System Department of Health Sciences: Discipline (MLT-04) (VIROLOGY &MYCOLOGY)Документ5 страницNcs University System Department of Health Sciences: Discipline (MLT-04) (VIROLOGY &MYCOLOGY)Habib UllahОценок пока нет
- 120Документ349 страниц120xdyj2005Оценок пока нет
- 1-Theory of Metal Cutting PDFДокумент144 страницы1-Theory of Metal Cutting PDFNithinArvindОценок пока нет
- 1414-Electric Room 1 Calculation Report Rev.02Документ28 страниц1414-Electric Room 1 Calculation Report Rev.02zakariaelrayesusaОценок пока нет
- Grade 7 Information Writing: The Bulldog: A Dog Like No OtherДокумент5 страницGrade 7 Information Writing: The Bulldog: A Dog Like No Otherapi-202727113Оценок пока нет
- NoahДокумент2 страницыNoahapi-302505193Оценок пока нет
- Astm D3078-02Документ3 страницыAstm D3078-02Geoff EricksonОценок пока нет
- 3rd Quarter Performance TaskДокумент3 страницы3rd Quarter Performance TaskJaime CrispinoОценок пока нет
- A Bilateral Subdural Hematoma Case Report 2165 7548.1000112 PDFДокумент2 страницыA Bilateral Subdural Hematoma Case Report 2165 7548.1000112 PDFPutra GagahОценок пока нет
- DalmatiaДокумент265 страницDalmatiaomissam2Оценок пока нет
- Gurps Fallout HandgunsДокумент1 страницаGurps Fallout HandgunsAndrew Scott100% (1)
- BS en 6100-3-2 Electromagnetic Compatibility (EMC)Документ12 страницBS en 6100-3-2 Electromagnetic Compatibility (EMC)Arun Jacob CherianОценок пока нет
- Relay Identification: Example CDG31FF002SACHДокумент5 страницRelay Identification: Example CDG31FF002SACHRohit RanaОценок пока нет
- Iso 3932 1976Документ8 страницIso 3932 1976NaveedОценок пока нет
- Effect of Toe Treatments On The Fatigue Resistance of Structural Steel WeldsДокумент12 страницEffect of Toe Treatments On The Fatigue Resistance of Structural Steel WeldsVicente Palazzo De MarinoОценок пока нет
- Text For Number 1-3: How To Make Passion Fruit Juice IngredientsДокумент4 страницыText For Number 1-3: How To Make Passion Fruit Juice Ingredientsakmal maulanaОценок пока нет
- Telmisartan, ISMNДокумент8 страницTelmisartan, ISMNDenise EspinosaОценок пока нет
- Standard MissileДокумент2 страницыStandard Missilemadox_3m100% (1)
- Water Treatment Lecture 4Документ34 страницыWater Treatment Lecture 4pramudita nadiahОценок пока нет
- ASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFДокумент5 страницASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFАртем ТитовОценок пока нет
- Alginate Impression MaterialДокумент92 страницыAlginate Impression MaterialrusschallengerОценок пока нет