Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Final Thesis - Aris PotliopoulosДокумент94 страницыFinal Thesis - Aris PotliopoulosCristinaОценок пока нет
- History and Philo of ScienceДокумент5 страницHistory and Philo of ScienceJan Oliver YaresОценок пока нет
- Brief Summary of Catalytic ConverterДокумент23 страницыBrief Summary of Catalytic ConverterjoelОценок пока нет
- Comparative Performance of Some Cattle Breeds Under Barani Conditions of PakistanДокумент4 страницыComparative Performance of Some Cattle Breeds Under Barani Conditions of PakistanMasood HassanОценок пока нет
- Intumescent Paint For Steel NZ - Coating - Co.nzДокумент8 страницIntumescent Paint For Steel NZ - Coating - Co.nzPeter ThomsonОценок пока нет
- Sw34 Religion, Secularism and The Environment by NasrДокумент19 страницSw34 Religion, Secularism and The Environment by Nasrbawah61455Оценок пока нет
- Class 12 Maths Project On Prime NumbersДокумент13 страницClass 12 Maths Project On Prime Numbersanon_3835245630% (1)
- L GH Catalog PullingДокумент60 страницL GH Catalog PullingLuis LuperdiОценок пока нет
- Banachek UnlimitedДокумент34 страницыBanachek UnlimitedserenaОценок пока нет
- Fama Fraternitatis Rosae Crucis PDFДокумент2 страницыFama Fraternitatis Rosae Crucis PDFJudy50% (2)
- Physics 101Документ21 страницаPhysics 101Kuna KunavathiОценок пока нет
- Illuminati TruthsДокумент27 страницIlluminati TruthsDonnaveo ShermanОценок пока нет
- Engineering Structures: C.X. Dong, A.K.H. Kwan, J.C.M. HoДокумент14 страницEngineering Structures: C.X. Dong, A.K.H. Kwan, J.C.M. HoElieser SinagaОценок пока нет
- Reloved - October 2015Документ116 страницReloved - October 2015Barron Fields67% (3)
- Greater Occipital Nerve Block: Pain ManagementДокумент3 страницыGreater Occipital Nerve Block: Pain Managementkillingeyes177Оценок пока нет
- Shell Gadus: Designed To Do More. Just Like Our Greases - Shell GadusДокумент2 страницыShell Gadus: Designed To Do More. Just Like Our Greases - Shell Gadusperi irawanОценок пока нет
- Case StudyДокумент61 страницаCase StudyA GОценок пока нет
- Apcotide 1000 pc2782Документ1 страницаApcotide 1000 pc2782hellmanyaОценок пока нет
- Abnormalities of Placenta, Amniotic Fluid and Cord: Prepared By, B. Ezhilarasi, Nursing TutorДокумент21 страницаAbnormalities of Placenta, Amniotic Fluid and Cord: Prepared By, B. Ezhilarasi, Nursing TutorGopala KrishnanОценок пока нет
- Relationships, 365 Day Devotional Mylesunroe 377pgДокумент377 страницRelationships, 365 Day Devotional Mylesunroe 377pgEla100% (7)
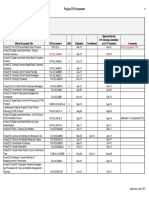
- Approved Project 25 StandardsДокумент5 страницApproved Project 25 StandardsepidavriosОценок пока нет
- Egt Margen From The Best ArticalДокумент6 страницEgt Margen From The Best ArticalakeelОценок пока нет
- Overall Method StatementДокумент33 страницыOverall Method Statementsaranga100% (1)
- PAG7.1 Student The Effects of Antibiotics On Microbial Growth - v0.3Документ3 страницыPAG7.1 Student The Effects of Antibiotics On Microbial Growth - v0.3Habib UddinОценок пока нет
- ELIDA Products CatalogueДокумент37 страницELIDA Products CatalogueAbhishek AgarwalОценок пока нет
- Complete Processing Lines For Extruded Pet FoodДокумент13 страницComplete Processing Lines For Extruded Pet FoodденисОценок пока нет
- Kodak Easyshare Z712 Is Zoom Digital Camera: User'S GuideДокумент75 страницKodak Easyshare Z712 Is Zoom Digital Camera: User'S GuideIronko PepeОценок пока нет
- RUKUS April 2011Документ40 страницRUKUS April 2011RUKUS Magazine100% (2)
- Dialog Bahasa InggirsДокумент2 страницыDialog Bahasa InggirsKeRtha NeghaRaОценок пока нет