Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Shutter Island PDFДокумент3 страницыShutter Island PDFJay Campbell67% (3)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Non Surgical Fat ReductionДокумент12 страницNon Surgical Fat ReductionadeОценок пока нет
- Sony DSC-F828 Service ManualДокумент287 страницSony DSC-F828 Service ManualgndleeОценок пока нет
- Aegeus Case StudyДокумент2 страницыAegeus Case StudyeftychidisОценок пока нет
- Exogenous Ochronosis Treated With CO2 LaserДокумент3 страницыExogenous Ochronosis Treated With CO2 LaseradeОценок пока нет
- Exogenous Ochronosis-Successful Outcome After Treatment QS NdYAG LaserДокумент6 страницExogenous Ochronosis-Successful Outcome After Treatment QS NdYAG LaseradeОценок пока нет
- Neuroprotective and Anti-Aging Potentials of Essential Oils From Aromatic and Medicinal PlantsДокумент16 страницNeuroprotective and Anti-Aging Potentials of Essential Oils From Aromatic and Medicinal PlantsLuisa FernandaОценок пока нет
- TX of StriaeДокумент13 страницTX of StriaeadeОценок пока нет
- Ablative and Non AblativeF Acial Skin RejuvenationДокумент241 страницаAblative and Non AblativeF Acial Skin RejuvenationadeОценок пока нет
- Catalog Alat PDFДокумент22 страницыCatalog Alat PDFadeОценок пока нет
- Diagnosis and Treatment of PCOSДокумент8 страницDiagnosis and Treatment of PCOSChlarasintaBenyaminОценок пока нет
- WJC 7 204 PDFДокумент12 страницWJC 7 204 PDFadeОценок пока нет
- Sympathetic Nervous System Overactivity and Its Role in The Development of Cardiovascular DiseaseДокумент45 страницSympathetic Nervous System Overactivity and Its Role in The Development of Cardiovascular DiseaseadeОценок пока нет
- Updates in Medical Skin Care: Advances in Cosmetic SurgeryДокумент7 страницUpdates in Medical Skin Care: Advances in Cosmetic SurgeryadeОценок пока нет
- Heart Rate Variability: A Noninvasive Electrocardiographic Method To Measure The Autonomic Nervous SystemДокумент10 страницHeart Rate Variability: A Noninvasive Electrocardiographic Method To Measure The Autonomic Nervous SystemadeОценок пока нет
- Role of The Autonomic Nervous System in Modulating Cardiac ArrhythmiasДокумент18 страницRole of The Autonomic Nervous System in Modulating Cardiac ArrhythmiasadeОценок пока нет
- Role of The Autonomic Nervous System in Modulating Cardiac ArrhythmiasДокумент18 страницRole of The Autonomic Nervous System in Modulating Cardiac ArrhythmiasadeОценок пока нет
- Vit A Dan e Pada KehamilanДокумент13 страницVit A Dan e Pada KehamilanadeОценок пока нет
- WJC 7 204 PDFДокумент12 страницWJC 7 204 PDFadeОценок пока нет
- Journal Pone 0200799Документ13 страницJournal Pone 0200799adeОценок пока нет
- The Human Sympathetic Nervous System: Its Relevance in Hypertension and Heart FailureДокумент10 страницThe Human Sympathetic Nervous System: Its Relevance in Hypertension and Heart FailureadeОценок пока нет
- Jcem 4565Документ28 страницJcem 4565Cota AncutaОценок пока нет
- The Autonomic Nervous System and Cardiovascular Health and DiseaseДокумент3 страницыThe Autonomic Nervous System and Cardiovascular Health and DiseaseadeОценок пока нет
- Jurnal KardioДокумент11 страницJurnal KardioadeОценок пока нет
- Jcem 4565Документ28 страницJcem 4565Cota AncutaОценок пока нет
- Neuroprotective and Anti-Aging Potentials of Essential Oils From Aromatic and Medicinal PlantsДокумент16 страницNeuroprotective and Anti-Aging Potentials of Essential Oils From Aromatic and Medicinal PlantsLuisa FernandaОценок пока нет
- Alfa Toco Ferol Vitamina eДокумент9 страницAlfa Toco Ferol Vitamina eBetty Garrido SeoaneОценок пока нет
- Vitamin B PDFДокумент19 страницVitamin B PDFadeОценок пока нет
- Manajemen Sepsis - SSCДокумент8 страницManajemen Sepsis - SSCDeborah Bravian TairasОценок пока нет
- Citicoline (Qureshi)Документ15 страницCiticoline (Qureshi)Lalalala Gabriella KristianiОценок пока нет
- ASIM Issue 4 10Dp904 907 PDFДокумент4 страницыASIM Issue 4 10Dp904 907 PDFadeОценок пока нет
- Current Guidelines For The Management of Asthma in Young Children PDFДокумент13 страницCurrent Guidelines For The Management of Asthma in Young Children PDFadeОценок пока нет
- Content: Standard Operating Procedure (SOP) Maintenance of A Light MicroscopeДокумент8 страницContent: Standard Operating Procedure (SOP) Maintenance of A Light MicroscopechyeebiyooОценок пока нет
- Share Myopia Mcqs'sДокумент4 страницыShare Myopia Mcqs'sshumaila khan50% (2)
- Instruments Used in Questioned Documents ExaminationДокумент11 страницInstruments Used in Questioned Documents ExaminationJENNIFER PADIERNOSОценок пока нет
- Observing Starch Grain in Potato ExperimentДокумент1 страницаObserving Starch Grain in Potato Experimentsadiqah mushtaqОценок пока нет
- Ckla GK U2 Teahers GuideДокумент114 страницCkla GK U2 Teahers Guideapi-286549827Оценок пока нет
- Check List For Monitoring To Toll Plaza by IeДокумент2 страницыCheck List For Monitoring To Toll Plaza by IeAnonymous eKt1FCD100% (1)
- HAC HFW1509TLM IL A - Datasheet - 20220817Документ3 страницыHAC HFW1509TLM IL A - Datasheet - 20220817citracandikaОценок пока нет
- Encyclopedia of Film Techniques and Technologies, TECHNÈS - ParcoursДокумент19 страницEncyclopedia of Film Techniques and Technologies, TECHNÈS - ParcoursPablo PlaОценок пока нет
- Test Bank For Introductory Statistics 9 e 9th Edition 0321897196Документ38 страницTest Bank For Introductory Statistics 9 e 9th Edition 0321897196petaledrevealer155f100% (13)
- L9 Initial MPMVA BVSДокумент25 страницL9 Initial MPMVA BVSDjbr MohОценок пока нет
- Type 2 Conditional Grammar: ACTIVITY 4: The Zero ConditionalДокумент2 страницыType 2 Conditional Grammar: ACTIVITY 4: The Zero ConditionalJose Luis Garza Viera0% (1)
- Gemalto - Customer Presentation - Part 2 - LFIS - Functionalities OverviewДокумент15 страницGemalto - Customer Presentation - Part 2 - LFIS - Functionalities OverviewJoséОценок пока нет
- Toronto Cataract ConferenceДокумент6 страницToronto Cataract ConferenceDee Margaux SantiagoОценок пока нет
- Claymation AssignmentДокумент7 страницClaymation AssignmentGrayson AllensworthОценок пока нет
- Film Techniques in Broadcast JournalismДокумент12 страницFilm Techniques in Broadcast Journalismapi-545022848Оценок пока нет
- Field of ViewДокумент11 страницField of ViewFlorian LindnerОценок пока нет
- Descriptive Essay StructureДокумент3 страницыDescriptive Essay StructureafabifazvОценок пока нет
- Instructional PhotographyLECTURE - 2 (Recovered)Документ46 страницInstructional PhotographyLECTURE - 2 (Recovered)Lara ZuñigaОценок пока нет
- Rhetorical Analysis (Sally Mann's Candy Cigarette)Документ4 страницыRhetorical Analysis (Sally Mann's Candy Cigarette)asanche8100% (1)
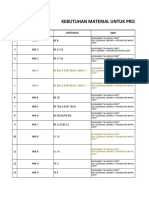
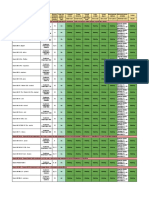
- Rap Material PltuДокумент9 страницRap Material PltuReggy GantiraОценок пока нет
- How To Get The Best Out of Your PopДокумент8 страницHow To Get The Best Out of Your PopTHIRDVISION STUDIOSОценок пока нет
- ĐỀ SỐ 04 HSG ANH 9Документ16 страницĐỀ SỐ 04 HSG ANH 9Thuy AnhОценок пока нет
- Electron MicroscopyДокумент35 страницElectron MicroscopyAwais FaizyОценок пока нет
- Answer The Following in Your Science Notebook. ANSWER ONLY Part I: Study The Refraction of Light Diagram Below and Answer The Questions That FollowsДокумент3 страницыAnswer The Following in Your Science Notebook. ANSWER ONLY Part I: Study The Refraction of Light Diagram Below and Answer The Questions That FollowsMariez BanlutaОценок пока нет
- Forensic 1 Module 3 NotesДокумент10 страницForensic 1 Module 3 Notesgenelord opallaОценок пока нет
- Google Camera by B-S-GДокумент16 страницGoogle Camera by B-S-GChakiem SpeederОценок пока нет
- Structural Parts of A Light and Electron Microscope and Their FunctionsДокумент3 страницыStructural Parts of A Light and Electron Microscope and Their FunctionsBonagua Felix MayoОценок пока нет