Вам также может понравиться
- A New History of Vaccines for Infectious Diseases: Immunization - Chance and NecessityОт EverandA New History of Vaccines for Infectious Diseases: Immunization - Chance and NecessityОценок пока нет
- CALDERON Bacteriology Worksheet With AnswersДокумент3 страницыCALDERON Bacteriology Worksheet With AnswersJames Belgira TamayoОценок пока нет
- Abdul CadarДокумент4 страницыAbdul CadarVitta Kusma WijayaОценок пока нет
- Parasitic Diseases OMSДокумент13 страницParasitic Diseases OMSlacmftcОценок пока нет
- Acinetobacter Neonatal Infection. Mortality Associated Risk FactorsДокумент8 страницAcinetobacter Neonatal Infection. Mortality Associated Risk FactorsAli Faisal SaleemОценок пока нет
- Acinetobacter BaumanniiДокумент12 страницAcinetobacter BaumanniiKenneth Smith IIОценок пока нет
- 2016 Piis1201971216310761Документ4 страницы2016 Piis1201971216310761Soraya Eugenia Morales LópezОценок пока нет
- FactSheet AcinetobacterДокумент2 страницыFactSheet AcinetobacterDrashua AshuaОценок пока нет
- Medscape Quiz For MicroДокумент17 страницMedscape Quiz For MicroJennifer GuilarteОценок пока нет
- Acinetobacter BaumanniiДокумент53 страницыAcinetobacter BaumanniiLaboratorium BorromeusОценок пока нет
- Prospective Study in A Porcine Model of Sarcoptes Scabiei Indicates The Association of Th2 and Th17 Pathways With The Clinical Severity of ScabiesДокумент17 страницProspective Study in A Porcine Model of Sarcoptes Scabiei Indicates The Association of Th2 and Th17 Pathways With The Clinical Severity of ScabiespunyayaОценок пока нет
- Cjim 12 232Документ4 страницыCjim 12 232Rahma Tiana PutriОценок пока нет
- Jpids Pis043 FullДокумент3 страницыJpids Pis043 FullRani Eva DewiОценок пока нет
- Anuradha NДокумент4 страницыAnuradha NIJAMОценок пока нет
- JURNAL AmoebiasisДокумент4 страницыJURNAL Amoebiasisdokteradhit891438Оценок пока нет
- Scabies Mites Alter The Skin Microbiome and PromoteДокумент13 страницScabies Mites Alter The Skin Microbiome and Promotemohammed bouchibaОценок пока нет
- TreatmentДокумент3 страницыTreatmentNarasimharao HarnoorОценок пока нет
- The Stethoscope As A Vector of Infectious Diseases in The Paediatric DivisionДокумент3 страницыThe Stethoscope As A Vector of Infectious Diseases in The Paediatric DivisionAlagarsamy GОценок пока нет
- Crossm: The Brief Case: Disseminated Histoplasma Capsulatum in A Patient With Newly Diagnosed HIV Infection/AIDSДокумент5 страницCrossm: The Brief Case: Disseminated Histoplasma Capsulatum in A Patient With Newly Diagnosed HIV Infection/AIDSanggoenzОценок пока нет
- A.baumanii in ChildrenДокумент11 страницA.baumanii in ChildrenIvana ErakovicОценок пока нет
- Fatal Subdural Empyema Caused by Streptococcus Constellatus and Actinomyces Viscosus in A Childdcase ReportДокумент3 страницыFatal Subdural Empyema Caused by Streptococcus Constellatus and Actinomyces Viscosus in A Childdcase ReportwawaningОценок пока нет
- Case Study of MastitisДокумент2 страницыCase Study of MastitisJoule PeirreОценок пока нет
- A.baumanii Colonization vs. InfectionДокумент12 страницA.baumanii Colonization vs. InfectionIvana ErakovicОценок пока нет
- International Journal of Infectious DiseasesДокумент4 страницыInternational Journal of Infectious DiseasesSABA YOUNASОценок пока нет
- Causative Agent:: M. Tuberculosis Has An Unusual, Waxy Coating On The Cell Surface (Primarily Mycolic Acid)Документ4 страницыCausative Agent:: M. Tuberculosis Has An Unusual, Waxy Coating On The Cell Surface (Primarily Mycolic Acid)Ervin BatangosoОценок пока нет
- Bacteremia Involving The Streptococcus Milleri Group Analysis of 19 CasesДокумент10 страницBacteremia Involving The Streptococcus Milleri Group Analysis of 19 CasesAmir addaniОценок пока нет
- Why and How Vaccines WorkДокумент6 страницWhy and How Vaccines WorkAniruddha RoyОценок пока нет
- Should All Bacteraemia Be Treated? A Case Report of An Immunocompetent Patient With Campylobacter Upsaliensis BacteraemiaДокумент4 страницыShould All Bacteraemia Be Treated? A Case Report of An Immunocompetent Patient With Campylobacter Upsaliensis Bacteraemiaps piasОценок пока нет
- Antimicrobial Resistance in Hospital-Acquired Gram-Negative Bacterial InfectionsДокумент9 страницAntimicrobial Resistance in Hospital-Acquired Gram-Negative Bacterial InfectionsAlina BanciuОценок пока нет
- Hospital Pediatrics 2011 McCulloh 52 4Документ5 страницHospital Pediatrics 2011 McCulloh 52 4Denso Antonius LimОценок пока нет
- Lakew 2013Документ4 страницыLakew 2013Ali AbidОценок пока нет
- Course Title: Ruminant and Non-Ruminant Preventive MedicineДокумент32 страницыCourse Title: Ruminant and Non-Ruminant Preventive MedicineFarhan NobelОценок пока нет
- Aborto Septico 2020Документ5 страницAborto Septico 2020Adrian Pardo VillegasОценок пока нет
- Microbiological Profile of Bronchoalveolar Lavage in Patients With Nosocomial Pneumonia in Neonatal Intensive Care UnitДокумент4 страницыMicrobiological Profile of Bronchoalveolar Lavage in Patients With Nosocomial Pneumonia in Neonatal Intensive Care UnitIJAR JOURNALОценок пока нет
- Diphtheria Investigation GuidelineДокумент20 страницDiphtheria Investigation GuidelineIslammiyah Dewi YuniantiОценок пока нет
- BMBL5 Sect VIII D, 0 PDFДокумент5 страницBMBL5 Sect VIII D, 0 PDFshaifОценок пока нет
- Journal 3Документ11 страницJournal 3margareth silaenОценок пока нет
- Infections, Immunity and Forensics: A Extensions 6.7 To 6.11Документ4 страницыInfections, Immunity and Forensics: A Extensions 6.7 To 6.11Saifulahmed49Оценок пока нет
- Klebsiella Pneumoniae Pathogenesis: Etiology/BacteriologyДокумент4 страницыKlebsiella Pneumoniae Pathogenesis: Etiology/Bacteriologysuper cute100% (1)
- datapage,+IJIC A 21712 OДокумент9 страницdatapage,+IJIC A 21712 OFizza MaryamОценок пока нет
- Microbiology: of AbscessДокумент5 страницMicrobiology: of AbscessJuan SetiajiОценок пока нет
- Highly Effective Against EsblДокумент9 страницHighly Effective Against Esblgaurav rawalОценок пока нет
- Molecular Characterisation of An Acinetobacter Baumannii OutbreakДокумент9 страницMolecular Characterisation of An Acinetobacter Baumannii OutbreakRamón RicardoОценок пока нет
- Review of Known and Unknown Facts of Klebsiella Pneumoniae and Its Relationship With AntibioticsДокумент8 страницReview of Known and Unknown Facts of Klebsiella Pneumoniae and Its Relationship With AntibioticsPhuong NguyenОценок пока нет
- 15empirical Treatment of Neonatal Sepsis - Are The Current Guidelines AdequateДокумент6 страниц15empirical Treatment of Neonatal Sepsis - Are The Current Guidelines Adequategitano1225Оценок пока нет
- Compliationof PuerperimДокумент27 страницCompliationof PuerperimSuman GuptaОценок пока нет
- M.tuberculosis Complex, CB-NAAT, Abscess, Acid Fast BacilliДокумент5 страницM.tuberculosis Complex, CB-NAAT, Abscess, Acid Fast BacilliMosesОценок пока нет
- Clinical Spectrum and Antibiogram of Acinetobacter Infections in Children Study From A Tertiary Care Centre, IndiaДокумент12 страницClinical Spectrum and Antibiogram of Acinetobacter Infections in Children Study From A Tertiary Care Centre, IndiaInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- MICP CaseДокумент5 страницMICP CaseRALPH EDELWEISS GAPASINОценок пока нет
- Republic of IraqДокумент8 страницRepublic of Iraqbahaa husienОценок пока нет
- Nosocomial Infections in Pediatric Intensive Care UnitДокумент6 страницNosocomial Infections in Pediatric Intensive Care UnitEditor IJTSRDОценок пока нет
- Cereus 3Документ19 страницCereus 3Natalia DuqueОценок пока нет
- Acquired Hospital: InfectionДокумент3 страницыAcquired Hospital: Infectionnayem hossainОценок пока нет
- Infectious Diseases of The Female Genital TractДокумент1 111 страницInfectious Diseases of The Female Genital TractJohn Ntokos100% (2)
- Chlamydia, MycoplasmaДокумент8 страницChlamydia, MycoplasmaMBMОценок пока нет
- Created By: Michael Anthony C. Macaballug, R.NДокумент115 страницCreated By: Michael Anthony C. Macaballug, R.NRubyFranzCabangbang-QuilbanОценок пока нет
- Presentation On: Pueperal Sepsis: Submitted To: Sandhya Maam Submitted By: Dhana BC Kismita Rai BSC 3 YearДокумент31 страницаPresentation On: Pueperal Sepsis: Submitted To: Sandhya Maam Submitted By: Dhana BC Kismita Rai BSC 3 YearRumi Maharjan100% (1)
- VREAbreifreviewДокумент6 страницVREAbreifreviewVini KastilaОценок пока нет
- Microbiology IIIДокумент34 страницыMicrobiology IIIsafemind100% (1)
- Serkom - UNTAR FebДокумент2 страницыSerkom - UNTAR FebSteven HerbertОценок пока нет
- Psyllium-Curr Topics Nutrac ResДокумент10 страницPsyllium-Curr Topics Nutrac ResSteven HerbertОценок пока нет
- Poster Kusta KKДокумент6 страницPoster Kusta KKSteven HerbertОценок пока нет
- Abdomen Radiography: Daniel JayaprakashДокумент27 страницAbdomen Radiography: Daniel JayaprakashSteven HerbertОценок пока нет
- Plain Picture in Acute Abdomen: Moderator-Dr (Prof) - R. K. GogoiДокумент127 страницPlain Picture in Acute Abdomen: Moderator-Dr (Prof) - R. K. GogoiSteven HerbertОценок пока нет
- Serkom - UNTAR FebДокумент2 страницыSerkom - UNTAR FebSteven HerbertОценок пока нет
- Data DK Teluk Naga 1Документ10 страницData DK Teluk Naga 1Steven HerbertОценок пока нет
- Dash Board Maret 2015Документ151 страницаDash Board Maret 2015Steven HerbertОценок пока нет
- SumberДокумент1 страницаSumberSteven HerbertОценок пока нет
- Daftar PustakaДокумент2 страницыDaftar PustakaSteven HerbertОценок пока нет
- Breech Presentation and DeliveryДокумент7 страницBreech Presentation and DeliverySteven Herbert0% (1)
- Jurnal B.ingДокумент9 страницJurnal B.ingFarel Isbister Stewart GurningОценок пока нет
- Breech Presentation and DeliveryДокумент7 страницBreech Presentation and DeliverySteven Herbert0% (1)
- TobaДокумент4 страницыTobaSteven HerbertОценок пока нет
- Alpha Disc LogДокумент1 страницаAlpha Disc LogSteven HerbertОценок пока нет
- 104 313 1 PBДокумент3 страницы104 313 1 PBSteven HerbertОценок пока нет
- Single PilДокумент12 страницSingle PilSteven HerbertОценок пока нет
- 104 313 1 PBДокумент3 страницы104 313 1 PBSteven HerbertОценок пока нет
- FTPДокумент8 страницFTPSteven HerbertОценок пока нет
- Single PilДокумент12 страницSingle PilSteven HerbertОценок пока нет
- Normal SalineДокумент5 страницNormal SalineSteven HerbertОценок пока нет
- TobaДокумент4 страницыTobaSteven HerbertОценок пока нет
- Clin Infect Dis. 2007 Sungkanuparph 447 52Документ6 страницClin Infect Dis. 2007 Sungkanuparph 447 52Steven HerbertОценок пока нет
- Sputum Colour: A Useful Clinical Tool in Non-Cystic Fibrosis BronchiectasisДокумент4 страницыSputum Colour: A Useful Clinical Tool in Non-Cystic Fibrosis BronchiectasisSteven HerbertОценок пока нет
- Jurnal Kegiatan GeriatriДокумент2 страницыJurnal Kegiatan GeriatriSteven HerbertОценок пока нет
- 10 1 1 272 3226Документ10 страниц10 1 1 272 3226Steven HerbertОценок пока нет
- 104 313 1 PBДокумент3 страницы104 313 1 PBSteven HerbertОценок пока нет
- Belkin User LogДокумент1 страницаBelkin User LogSteven HerbertОценок пока нет
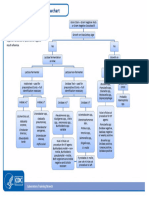
- Aerobic Gram Negative Rods FlowchartДокумент1 страницаAerobic Gram Negative Rods FlowchartKeithОценок пока нет
- Assignment 1Документ5 страницAssignment 1Patty ReyesОценок пока нет
- Mathematical Model For Malaria TransmissionДокумент32 страницыMathematical Model For Malaria TransmissionAunisaliОценок пока нет
- Vector ControlДокумент19 страницVector ControlrodelagapitoОценок пока нет
- MrASHISHDUBEY 29Y MaleДокумент2 страницыMrASHISHDUBEY 29Y MaleNisha DubeyОценок пока нет
- Table of Parasited (Parasitology)Документ9 страницTable of Parasited (Parasitology)abcОценок пока нет
- Essentials of Business Law 10th Edition Liuzzo Solutions Manual Full Chapter PDFДокумент37 страницEssentials of Business Law 10th Edition Liuzzo Solutions Manual Full Chapter PDFquandiendjv100% (15)
- MCQ DermatologyДокумент42 страницыMCQ Dermatologydraik71100% (5)
- Ahmed MNCH, Basics Health Care 2021Документ6 страницAhmed MNCH, Basics Health Care 2021Rozen TarequeОценок пока нет
- Acute GlomerulonephritisДокумент32 страницыAcute GlomerulonephritisEzekiel moraraОценок пока нет
- Microbiology and Genetics Course Outline Spring 2014Документ3 страницыMicrobiology and Genetics Course Outline Spring 2014api-244509569Оценок пока нет
- Rita I.T ReportДокумент30 страницRita I.T ReportAugustineОценок пока нет
- Handwahing DetailsДокумент2 страницыHandwahing DetailsLee ShaneОценок пока нет
- MATERIAL DE APOYO 2P-2Q 9th-SCIENCE 22-23Документ34 страницыMATERIAL DE APOYO 2P-2Q 9th-SCIENCE 22-23kleverpОценок пока нет
- 2014 Editorial June 2014Документ20 страниц2014 Editorial June 2014panniyin selvanОценок пока нет
- Outbreak Investigation Case Scenarios-PHASE III-SDL, 15-17.05.2023-1Документ13 страницOutbreak Investigation Case Scenarios-PHASE III-SDL, 15-17.05.2023-1srinidhi premkumarОценок пока нет
- Clinical ParasitologyДокумент11 страницClinical ParasitologySky QuizonОценок пока нет
- Form B Microbe Mission Division B Exam: Symbiotic Archaea BacteriaДокумент3 страницыForm B Microbe Mission Division B Exam: Symbiotic Archaea BacteriasandeeptaraОценок пока нет
- Batangas Communicable Dse Post Test SCДокумент2 страницыBatangas Communicable Dse Post Test SCcianm1143Оценок пока нет
- Literature ReviewДокумент2 страницыLiterature ReviewFaith Arpon AbogandaОценок пока нет
- The Use of Drains in Oral and Maxillofacial SurgeryДокумент4 страницыThe Use of Drains in Oral and Maxillofacial SurgeryAmit Date100% (2)
- Responsible AIDS and Becoming Human:: Faculty of Arts and PhilosophyДокумент91 страницаResponsible AIDS and Becoming Human:: Faculty of Arts and PhilosophyJuan Angel CiarloОценок пока нет
- School Contingency Plan For The Emerging and Re Emerging DiseasesДокумент47 страницSchool Contingency Plan For The Emerging and Re Emerging DiseasesWilson Jan AlcopraОценок пока нет
- Nursing CompetencyДокумент3 страницыNursing Competencyjerimiah_manzonОценок пока нет
- State Entity Employee #2: Veritext Legal Solutions 212-267-6868 516-608-2400Документ209 страницState Entity Employee #2: Veritext Legal Solutions 212-267-6868 516-608-2400cbs6albanyОценок пока нет
- JSA-001 Site Preparation & DevelopmentДокумент2 страницыJSA-001 Site Preparation & Developmentba ratnaparkhe50% (2)
- Otitis MediaДокумент5 страницOtitis MediaFajar NurrachmanОценок пока нет
- Scitech ReviewerДокумент2 страницыScitech ReviewerMARCH PHOTOS 2022Оценок пока нет
- MRSA in Septic ArthritisДокумент2 страницыMRSA in Septic ArthritisAmira AlmutairiОценок пока нет
- Caso 2 Sun Orchard Salmonella Outbreak 2023Документ2 страницыCaso 2 Sun Orchard Salmonella Outbreak 2023ÑehОценок пока нет