Вам также может понравиться
- MC Calandar - 2019 20Документ9 страницMC Calandar - 2019 20Adal ArasuОценок пока нет
- EIE101R01: Basic Electronics Engineering: Textbook and MaterialsДокумент7 страницEIE101R01: Basic Electronics Engineering: Textbook and MaterialsAdal ArasuОценок пока нет
- EIE101R01: Basic Electronics Engineering: Textbook and MaterialsДокумент9 страницEIE101R01: Basic Electronics Engineering: Textbook and MaterialsAdal ArasuОценок пока нет
- EIE101R01: Basic Electronics Engineering: Textbook and MaterialsДокумент14 страницEIE101R01: Basic Electronics Engineering: Textbook and MaterialsAdal ArasuОценок пока нет
- EIE101R01: Basic Electronics Engineering: Textbook and MaterialsДокумент6 страницEIE101R01: Basic Electronics Engineering: Textbook and MaterialsAdal ArasuОценок пока нет
- Out PDFДокумент107 страницOut PDFAdal ArasuОценок пока нет
- Publish2012 PDFДокумент1 страницаPublish2012 PDFAdal ArasuОценок пока нет
- EIE 101R01: Basic Electronics EngineeringДокумент20 страницEIE 101R01: Basic Electronics EngineeringAdal ArasuОценок пока нет
- "Stag Jump" Within The Context of ImpactДокумент8 страниц"Stag Jump" Within The Context of ImpactAdal ArasuОценок пока нет
- Lecture 2Документ39 страницLecture 2Adal ArasuОценок пока нет
- J Section Time Table PDFДокумент2 страницыJ Section Time Table PDFAdal ArasuОценок пока нет
- Ae Lab Ivsem EceДокумент60 страницAe Lab Ivsem EceNavneet KumarОценок пока нет
- 1st Yr Sections & Halls DetailsДокумент1 страница1st Yr Sections & Halls DetailsAdal ArasuОценок пока нет
- Basic Electronics Engineering Experiments (40Документ47 страницBasic Electronics Engineering Experiments (40Adal ArasuОценок пока нет
- Exercise 1Документ22 страницыExercise 1Adal Arasu100% (1)
- BC 107Документ3 страницыBC 107ganga_ch1Оценок пока нет
- Lecture 2Документ39 страницLecture 2Adal ArasuОценок пока нет
- Dr. K. Adalarasu: KA - MIT - Unit III - March, 2019, Sastra Deemed To Be UniversityДокумент41 страницаDr. K. Adalarasu: KA - MIT - Unit III - March, 2019, Sastra Deemed To Be UniversityAdal ArasuОценок пока нет
- RUSA CurriculumДокумент63 страницыRUSA CurriculumAdal ArasuОценок пока нет
- Sensors & Signal ConditioningДокумент11 страницSensors & Signal ConditioningAdal ArasuОценок пока нет
- Biomedical Instrumentation: Textbook and MaterialsДокумент25 страницBiomedical Instrumentation: Textbook and MaterialsAdal ArasuОценок пока нет
- Medical Imaging TechniquesДокумент6 страницMedical Imaging TechniquesAdal ArasuОценок пока нет
- Techniques of EMG Signal Analysis Detection, Processing, Classification andДокумент25 страницTechniques of EMG Signal Analysis Detection, Processing, Classification andTariq J FaridiОценок пока нет
- MC Calandar - 2019 20Документ9 страницMC Calandar - 2019 20Adal ArasuОценок пока нет
- Dr. K. Adalarasu: KA - MIT - Unit III - Feb, 2019, Sastra Deemed To UniversityДокумент28 страницDr. K. Adalarasu: KA - MIT - Unit III - Feb, 2019, Sastra Deemed To UniversityAdal ArasuОценок пока нет
- Dr. K. Adalarasu: KA - MIT - Unit III - March, 2019, Sastra Deemed To Be UniversityДокумент56 страницDr. K. Adalarasu: KA - MIT - Unit III - March, 2019, Sastra Deemed To Be UniversityAdal ArasuОценок пока нет
- EEG IBM Statisitc ResultsДокумент40 страницEEG IBM Statisitc ResultsAdal ArasuОценок пока нет
- Lecture Medical ImageДокумент80 страницLecture Medical ImageAdal ArasuОценок пока нет
- Biomedical Instrumentation: ReferenceДокумент23 страницыBiomedical Instrumentation: ReferenceAdal ArasuОценок пока нет
- Calender 2018-19Документ9 страницCalender 2018-19Adal ArasuОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- ¿Cómo Hacerlo?: Dr. Jorge Ramírez Medina, Dr. Guillermo Granados Ruíz EGADE Business SchoolДокумент17 страниц¿Cómo Hacerlo?: Dr. Jorge Ramírez Medina, Dr. Guillermo Granados Ruíz EGADE Business Schoolgalter6Оценок пока нет
- LTE Interview QuestionsДокумент10 страницLTE Interview QuestionsMahesh Pratap100% (1)
- Tiger AnddragonДокумент61 страницаTiger AnddragonAdil SiddiquiОценок пока нет
- 1729Документ52 страницы1729praj24083302Оценок пока нет
- Capacitor BanksДокумент49 страницCapacitor BanksAmal P RaviОценок пока нет
- L028 Me Dat 01 00122 001 00Документ8 страницL028 Me Dat 01 00122 001 00sivasan10006098Оценок пока нет
- Tes P 119 10 R0 PDFДокумент43 страницыTes P 119 10 R0 PDFAbin Meetu100% (4)
- CS 704 Socio-Emotional and Moral Development in Middle ChildhoodДокумент25 страницCS 704 Socio-Emotional and Moral Development in Middle ChildhoodPatricia PamintuanОценок пока нет
- Basic Facts For Homebooks Stage 7Документ3 страницыBasic Facts For Homebooks Stage 7api-311857762Оценок пока нет
- Ucc 900 Sor em Wpi 0001 - B01Документ73 страницыUcc 900 Sor em Wpi 0001 - B01JonesОценок пока нет
- Cropprotectionequipment-Rocker Sprayer - Specification (: Indian StandardДокумент9 страницCropprotectionequipment-Rocker Sprayer - Specification (: Indian Standardgini associatesОценок пока нет
- The Arcane Formulas or Mental AlchemyДокумент121 страницаThe Arcane Formulas or Mental AlchemyTim Boire100% (1)
- Check List of MossesДокумент319 страницCheck List of MossesAshen NirodyaОценок пока нет
- Enabling Keycloak Metrics - KeycloakДокумент3 страницыEnabling Keycloak Metrics - Keycloakhisyam darwisОценок пока нет
- 1.1 Thermodynamics 1Документ28 страниц1.1 Thermodynamics 1Lyan SantosОценок пока нет
- Toolbox Meeting Or, TBT (Toolbox TalkДокумент10 страницToolbox Meeting Or, TBT (Toolbox TalkHarold PonceОценок пока нет
- Grupo Stoncor Description - Stonhard Carboline Fibergrate PDFДокумент22 страницыGrupo Stoncor Description - Stonhard Carboline Fibergrate PDFAndres OsorioОценок пока нет
- DUPLICATE BILL TITLEДокумент8 страницDUPLICATE BILL TITLEMohammed AhmedОценок пока нет
- Exoskeleton Power Requirements Based on Human BiomechanicsДокумент54 страницыExoskeleton Power Requirements Based on Human Biomechanicsja2ja1Оценок пока нет
- Methanol Technical Data Sheet FactsДокумент1 страницаMethanol Technical Data Sheet FactsmkgmotleyОценок пока нет
- Zeal Institute of Manangement and Computer ApplicationДокумент4 страницыZeal Institute of Manangement and Computer ApplicationSONAL UTTARKARОценок пока нет
- Data Sheet: High-Speed DiodesДокумент7 страницData Sheet: High-Speed DiodesZoltán ÁgostonОценок пока нет
- Finimpianti Power EngДокумент2 страницыFinimpianti Power EngJosip GrlicaОценок пока нет
- Teodora Sarkizova: Certificate of AchievementДокумент2 страницыTeodora Sarkizova: Certificate of AchievementAbd El-RahmanОценок пока нет
- Topic 3Документ28 страницTopic 3Ashraf YusofОценок пока нет
- Adiabatic Production of Acetic AnhydrideДокумент7 страницAdiabatic Production of Acetic AnhydrideSunilParjapatiОценок пока нет
- 611k01 Kicatalog C Ka Us 1Документ8 страниц611k01 Kicatalog C Ka Us 1Ean LeeОценок пока нет
- Aw MD700 Manual G10 150706Документ73 страницыAw MD700 Manual G10 150706Heraldo Ulguim Luis OliveiraОценок пока нет
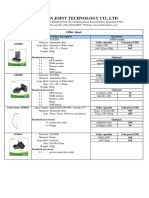
- Vehicle Tracker Offer SheetДокумент1 страницаVehicle Tracker Offer SheetBihun PandaОценок пока нет
- Advance Distributed ComputingДокумент2 страницыAdvance Distributed ComputingValia Centre of ExcellenceОценок пока нет