Вам также может понравиться
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsОт EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsОценок пока нет
- MAHSA University Global Mobility FormДокумент4 страницыMAHSA University Global Mobility FormEdgar ZetaОценок пока нет
- Instructions:: Part 1-Personal InformationДокумент7 страницInstructions:: Part 1-Personal InformationISLAND NATANYAОценок пока нет
- Clerk (Income Maintenance): Passbooks Study GuideОт EverandClerk (Income Maintenance): Passbooks Study GuideОценок пока нет
- Application Form For UNDP InternshipДокумент3 страницыApplication Form For UNDP InternshipRahul ChoudharyОценок пока нет
- Affidavit Support FormДокумент2 страницыAffidavit Support FormNofearmakОценок пока нет
- Application Form For UNDP InternshipДокумент3 страницыApplication Form For UNDP InternshipTamika Lee100% (1)
- Application InternsДокумент3 страницыApplication InternsAndam'zz Igomez HomiesОценок пока нет
- Application Form MTCP PDFДокумент8 страницApplication Form MTCP PDFrcalandriaОценок пока нет
- Guidelines and Application For Program AssistantДокумент3 страницыGuidelines and Application For Program AssistantSoundarayaОценок пока нет
- Bits ApplicationДокумент3 страницыBits ApplicationSugan RajОценок пока нет
- University of Engineering & Technology, Lahore: Application Form For Appointment/Fdp ScholarshipДокумент6 страницUniversity of Engineering & Technology, Lahore: Application Form For Appointment/Fdp ScholarshipUsama SanaullahОценок пока нет
- Akhil Dua UndpДокумент2 страницыAkhil Dua UndpAkhil DuaОценок пока нет
- Application For UNDP Internship ProgrammeДокумент3 страницыApplication For UNDP Internship ProgrammeFikri M IlyasaОценок пока нет
- Annexure-I Nomination/Registration Form - Applicants of Indian NationalityДокумент8 страницAnnexure-I Nomination/Registration Form - Applicants of Indian NationalityRohitОценок пока нет
- UNSW Scholarship Funding FormДокумент2 страницыUNSW Scholarship Funding FormkhuloodОценок пока нет
- Surety BondДокумент6 страницSurety BondBaba yagaОценок пока нет
- Mission 10-Appication Packet (Local Volunteers) PDFДокумент5 страницMission 10-Appication Packet (Local Volunteers) PDFLa Minor ChannelОценок пока нет
- UW Whitewater Medical Withdrawal FormДокумент3 страницыUW Whitewater Medical Withdrawal FormspencerОценок пока нет
- Health Systems Strengthening Participant Endorsement Form 2020Документ1 страницаHealth Systems Strengthening Participant Endorsement Form 2020Samuel WilliamsОценок пока нет
- Surety BondДокумент6 страницSurety Bondadharav malikОценок пока нет
- Authorization Form ParentДокумент1 страницаAuthorization Form ParentMikhel AlexanderОценок пока нет
- Observer Application: General Personal InformationДокумент3 страницыObserver Application: General Personal InformationDragomir IsabellaОценок пока нет
- SenateAppealsProforma2022 23v1Документ8 страницSenateAppealsProforma2022 23v12627057930Оценок пока нет
- TL Internship Application FormДокумент2 страницыTL Internship Application FormNazario Silva MonteiroОценок пока нет
- Japan-IMF Application FormДокумент7 страницJapan-IMF Application FormSirtufil LailaОценок пока нет
- Menu - 634705361804170000 - PG 2012 Application Form 20 April 2012Документ3 страницыMenu - 634705361804170000 - PG 2012 Application Form 20 April 2012Aakriti TripathiОценок пока нет
- Gyandeep Scholarship Terms With Declaration PDFДокумент4 страницыGyandeep Scholarship Terms With Declaration PDFReeshma NairОценок пока нет
- Official Seal or Stamp of Service/Employing Agency (If None, AДокумент2 страницыOfficial Seal or Stamp of Service/Employing Agency (If None, Aมดน้อย ผู้น่ารักОценок пока нет
- Surety Bond CCHN CHO Jan 2020 SessionДокумент5 страницSurety Bond CCHN CHO Jan 2020 SessionDivya MishraОценок пока нет
- 2019 Fellowship Programme For People of African Descent Application FormДокумент5 страниц2019 Fellowship Programme For People of African Descent Application FormHellen GomesОценок пока нет
- DUHS Electives Application FormДокумент4 страницыDUHS Electives Application FormAjayОценок пока нет
- PG 2014 Application FormДокумент3 страницыPG 2014 Application FormDeepak GaurОценок пока нет
- International Education Research Foundation, Inc.: Application For Nursing Licensure EvaluationДокумент4 страницыInternational Education Research Foundation, Inc.: Application For Nursing Licensure EvaluationZacky AzarragaОценок пока нет
- 000283Документ3 страницы000283Jonathan MartinezОценок пока нет
- Digitaljobsph Training ProgramДокумент3 страницыDigitaljobsph Training ProgramPrismagne Ai RotaquioОценок пока нет
- Application For Loan For Students at Gift UniversityДокумент3 страницыApplication For Loan For Students at Gift UniversityShahbaz MeharОценок пока нет
- AboutUs InternshipApplicationДокумент7 страницAboutUs InternshipApplicationpradeeptaxakОценок пока нет
- MOU AgreementДокумент8 страницMOU AgreementNelson Ticad CawilanОценок пока нет
- Application FormxcvДокумент5 страницApplication Formxcvbalamurugan_S1985Оценок пока нет
- FS Intern Requirements With SampleДокумент13 страницFS Intern Requirements With SampleJoseph Jucons C. SantosОценок пока нет
- Revised Certificate of CandidacyДокумент1 страницаRevised Certificate of CandidacyGomez, Jenna P.Оценок пока нет
- Joining InstructionsДокумент26 страницJoining InstructionsEugeneОценок пока нет
- Application Form For Migration To Nust: Intended Area of TransferДокумент6 страницApplication Form For Migration To Nust: Intended Area of TransferAbu HurairaОценок пока нет
- 2022 DJPH - GVA - Regionwide - Ifugao - LETTER OF ACCEPTANCE AND UNDERTAKING of TRAINEESДокумент3 страницы2022 DJPH - GVA - Regionwide - Ifugao - LETTER OF ACCEPTANCE AND UNDERTAKING of TRAINEESYvette MagatОценок пока нет
- Application Form - SHRI Academy - v2 - 15 Aug 2015Документ3 страницыApplication Form - SHRI Academy - v2 - 15 Aug 2015Janson GohОценок пока нет
- Vidyadeep Scholarship Terms - Fall DriveДокумент4 страницыVidyadeep Scholarship Terms - Fall DrivedhirkpОценок пока нет
- Marketing Mix of Automobile SectorДокумент29 страницMarketing Mix of Automobile SectorAbhineetSrivastavaОценок пока нет
- Cooperative Health Management Federation: Enrollment Application Form (Eaf)Документ2 страницыCooperative Health Management Federation: Enrollment Application Form (Eaf)Geraldine Daquipil TortalОценок пока нет
- Assam University Application Form 2015Документ7 страницAssam University Application Form 2015Live LawОценок пока нет
- F22 Forms PackageДокумент11 страницF22 Forms Packagelouise navorОценок пока нет
- ADEN - EP Student Evaluation Request 2021 Student LifeДокумент2 страницыADEN - EP Student Evaluation Request 2021 Student LifeAll CastilloОценок пока нет
- PRD 003429Документ1 страницаPRD 003429davidovoxoОценок пока нет
- PhilHealth ClaimForm2Документ2 страницыPhilHealth ClaimForm2La Lolls CruzОценок пока нет
- Scholarship & Study Grant Application Form: Any Results That Are Pending MUST Be Submitted As Soon As They Are ReleasedДокумент2 страницыScholarship & Study Grant Application Form: Any Results That Are Pending MUST Be Submitted As Soon As They Are ReleasedWilliamОценок пока нет
- Reg PackageДокумент12 страницReg PackageiqbarОценок пока нет
- PU Dmission FormДокумент7 страницPU Dmission FormChintan G JoshiОценок пока нет
- Memorandum of AgreementДокумент4 страницыMemorandum of AgreementRaymondGomezBlancoОценок пока нет
- STP Waiver - Doc Withkhh RevisionДокумент1 страницаSTP Waiver - Doc Withkhh RevisionMark PabalanОценок пока нет
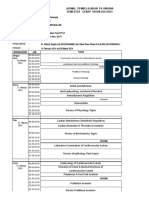
- Template KUPANG Kardiovaskular 2014Документ14 страницTemplate KUPANG Kardiovaskular 2014Sovian Anugrah Lumban GaolОценок пока нет
- Nama Produk Jumlah Harga Satuan SubtotalДокумент1 страницаNama Produk Jumlah Harga Satuan SubtotalSovian Anugrah Lumban GaolОценок пока нет
- The Lucid Interval Associated With Epidural Bleeding: Evolving UnderstandingДокумент2 страницыThe Lucid Interval Associated With Epidural Bleeding: Evolving UnderstandingSovian Anugrah Lumban GaolОценок пока нет
- HeunceutДокумент8 страницHeunceutSovian Anugrah Lumban GaolОценок пока нет
- Banking Adbl EnglishДокумент74 страницыBanking Adbl Englishdevi ghimireОценок пока нет
- PESTEL AnalysisДокумент2 страницыPESTEL AnalysisSayantan NandyОценок пока нет
- Eimco Elecon Initiating Coverage 04072016Документ19 страницEimco Elecon Initiating Coverage 04072016greyistariОценок пока нет
- IRDM Assignment-I PDFДокумент4 страницыIRDM Assignment-I PDFPiyush AggarwalОценок пока нет
- 5CT PDVSA em - 18!00!05 EnglishДокумент27 страниц5CT PDVSA em - 18!00!05 EnglishJuan Gutierrez100% (1)
- Vibration Absorbers: Scan This QR CodeДокумент4 страницыVibration Absorbers: Scan This QR CodeMohamed RaafatОценок пока нет
- Basic Customer Service SkillsДокумент90 страницBasic Customer Service SkillsGillian Delos ReyesОценок пока нет
- Shakespeare Ubd Unit PlanДокумент16 страницShakespeare Ubd Unit Planapi-239477809Оценок пока нет
- Police Log September 24, 2016Документ14 страницPolice Log September 24, 2016MansfieldMAPoliceОценок пока нет
- Keepa ApiДокумент55 страницKeepa ApiQazi Sohail AhmadОценок пока нет
- ProjectLookingGlassDeclassified PDFДокумент13 страницProjectLookingGlassDeclassified PDFAmi Ferguson83% (6)
- Ben ChanДокумент2 страницыBen ChanAlibabaОценок пока нет
- InvoiceДокумент1 страницаInvoiceKidambi SureshОценок пока нет
- Ahriman's Prophecy Walk ThroughДокумент106 страницAhriman's Prophecy Walk ThroughAngga Nata100% (1)
- Alburg-Caldwell Manor 1784-1826 Draft by Fay YoungДокумент3 страницыAlburg-Caldwell Manor 1784-1826 Draft by Fay YoungNancy Cunningham100% (1)
- Frankenstein ExtractДокумент1 страницаFrankenstein ExtractAnneОценок пока нет
- InflibnetДокумент3 страницыInflibnetSuhotra GuptaОценок пока нет
- Dpco 151223080520 PDFДокумент23 страницыDpco 151223080520 PDFSiva PrasadОценок пока нет
- Hyperinflation of Zimbabwe and The Lesson For Zimbabwe: Foreign Trade University Faculty of Banking and FinanceДокумент38 страницHyperinflation of Zimbabwe and The Lesson For Zimbabwe: Foreign Trade University Faculty of Banking and FinancePham Việt AnhОценок пока нет
- Site AnalysisДокумент4 страницыSite AnalysisS O NALОценок пока нет
- Chain Rule 3LNДокумент2 страницыChain Rule 3LNsaad khОценок пока нет
- Mil Tos (1ST Quarter)Документ3 страницыMil Tos (1ST Quarter)Rhea Carillo100% (14)
- Effect of Spent Engine Oil On The Internal Structure of Corchorus OlitoriusДокумент55 страницEffect of Spent Engine Oil On The Internal Structure of Corchorus Olitoriusanon_568621284Оценок пока нет
- WestIntroToSSB PDFДокумент100 страницWestIntroToSSB PDFnaval_05Оценок пока нет
- Macroeconomics Measurement: Part 2: Measurement of National IncomeДокумент13 страницMacroeconomics Measurement: Part 2: Measurement of National IncomeManish NepaliОценок пока нет
- Kbli 2017 - 1Документ50 страницKbli 2017 - 1Putri NadiaОценок пока нет
- SCI Annual Report 2017Документ32 страницыSCI Annual Report 2017The Seamen's Church Institute100% (2)
- ACCA Strategic Business Reporting (SBR) Workbook 2020Документ840 страницACCA Strategic Business Reporting (SBR) Workbook 2020Azba Nishath0% (1)
- Beamer Example: Ethan AltДокумент13 страницBeamer Example: Ethan AltManh Hoang VanОценок пока нет