Вам также может понравиться
- GoutДокумент10 страницGoutAmberОценок пока нет
- How To Treat: BackgroundДокумент6 страницHow To Treat: BackgroundmeeandsoeОценок пока нет
- Gout and Hyperuricemia: A Peer-Reviewed Bulletin For The Family PhysicianДокумент6 страницGout and Hyperuricemia: A Peer-Reviewed Bulletin For The Family PhysicianRhoda LicardoОценок пока нет
- Preview: Originally Published in Therapeutic Guidelines: Rheumatology, Version 2, 2010Документ2 страницыPreview: Originally Published in Therapeutic Guidelines: Rheumatology, Version 2, 2010Hannah CoОценок пока нет
- Part 1 Introduction BДокумент5 страницPart 1 Introduction BGeevee Naganag VentulaОценок пока нет
- Jop2010 608751Документ9 страницJop2010 608751Ahmad Ma'rufОценок пока нет
- Gout Term PaperДокумент8 страницGout Term Paperafmzubkeaydllz100% (1)
- GoutДокумент58 страницGoutusamadaifallahОценок пока нет
- Review On Treatment of Gout & HyperuricemiaДокумент11 страницReview On Treatment of Gout & HyperuricemiaMirza ProthikhaОценок пока нет
- Lyme DiseaseДокумент3 страницыLyme Diseaseanees jamalОценок пока нет
- Dalbeth 2021Документ13 страницDalbeth 2021Tensa ZangetsuОценок пока нет
- Gout: The Radiology and The Clinical ManifestationsДокумент9 страницGout: The Radiology and The Clinical ManifestationsDian YazmiatiОценок пока нет
- GoutДокумент12 страницGoutEarle Jimenez Niervo RN100% (1)
- Dissertation Rheumatoid ArthritisДокумент4 страницыDissertation Rheumatoid ArthritisFindSomeoneToWriteMyPaperUK100% (1)
- A2 Group 3 GOUTДокумент83 страницыA2 Group 3 GOUTArt Buenaventura0% (1)
- The Inflammatory ProcessДокумент7 страницThe Inflammatory ProcessDaniul ConuiОценок пока нет
- Case Scenario Nursing ProcessДокумент4 страницыCase Scenario Nursing ProcessJOANNA MAE ABIA SALOMONОценок пока нет
- Name: ID:: Madiha Sayed Nagy. 51859Документ12 страницName: ID:: Madiha Sayed Nagy. 51859drng48Оценок пока нет
- Artritis Inducida Por Depósito de CristalesДокумент10 страницArtritis Inducida Por Depósito de CristalesAlejandro GuzmánОценок пока нет
- Conventional Radiology ARTHRITISДокумент18 страницConventional Radiology ARTHRITISJojo LastОценок пока нет
- Differential diagnoses of joint pain scenarioДокумент9 страницDifferential diagnoses of joint pain scenarioNUR ZAMZAM AZIZAHОценок пока нет
- PseudoGout, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandPseudoGout, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Jurnal Gout EnglishДокумент8 страницJurnal Gout EnglishPutri ArtikaОценок пока нет
- Gout Is Usually Characterized by Recurrent Attacks ofДокумент14 страницGout Is Usually Characterized by Recurrent Attacks ofJimmy KusumaОценок пока нет
- Gout Is Usually Characterized by Recurrent Attacks ofДокумент15 страницGout Is Usually Characterized by Recurrent Attacks ofJimmy KusumaОценок пока нет
- Gout Is Usually Characterized by Recurrent Attacks ofДокумент17 страницGout Is Usually Characterized by Recurrent Attacks ofJimmy KusumaОценок пока нет
- Treating and Managing UveitisДокумент4 страницыTreating and Managing UveitisMoses Karanja Jr.Оценок пока нет
- Clinical PharmacyДокумент4 страницыClinical PharmacysadiaОценок пока нет
- Major Review: Glaucoma and UveitisДокумент10 страницMajor Review: Glaucoma and UveitisAlex MuñozОценок пока нет
- Seminar: Nicola Dalbeth, Anna L Gosling, Angelo Gaffo, Abhishek AbhishekДокумент13 страницSeminar: Nicola Dalbeth, Anna L Gosling, Angelo Gaffo, Abhishek AbhishekAslı Ecem AkyarОценок пока нет
- Rheumatoid Arthritis: Natural Approaches to Pain-Free LivingОт EverandRheumatoid Arthritis: Natural Approaches to Pain-Free LivingОценок пока нет
- Chapter 138: Management of Exophthalmos Thomas C. CalcaterraДокумент8 страницChapter 138: Management of Exophthalmos Thomas C. Calcaterrawisnu baskoroОценок пока нет
- Local Therapies For Inflammatory Eye Disease in Translation Past, Present and Future 2013Документ8 страницLocal Therapies For Inflammatory Eye Disease in Translation Past, Present and Future 2013Igor VainerОценок пока нет
- Rheumatoid Arthritis Associated Scleritis OPHTHALMOLOGY MCQSДокумент5 страницRheumatoid Arthritis Associated Scleritis OPHTHALMOLOGY MCQSkishorechandraОценок пока нет
- Rheumatoid Arthritis A Review and Dental Care ConsДокумент4 страницыRheumatoid Arthritis A Review and Dental Care ConsSofía TrianaОценок пока нет
- Classification and External Resources: Icd 10 Icd 9 Omim Diseasesdb Medlineplus 000422 Emedicine Patient Uk MeshДокумент9 страницClassification and External Resources: Icd 10 Icd 9 Omim Diseasesdb Medlineplus 000422 Emedicine Patient Uk MeshBecky NekesaОценок пока нет
- Gout and Othercrystal-Associated ArthropathiesДокумент31 страницаGout and Othercrystal-Associated ArthropathiesLia pramitaОценок пока нет
- Psoriasis JurnalДокумент24 страницыPsoriasis JurnaleverdroysОценок пока нет
- Kristal Artropati KuliahДокумент36 страницKristal Artropati KuliahRoby KieranОценок пока нет
- Episcleritis JournalДокумент9 страницEpiscleritis JournalDeaSafОценок пока нет
- Medicine Exam NotesДокумент211 страницMedicine Exam Notesjf65ky8f8tОценок пока нет
- Heart Valve Disease: State of the ArtОт EverandHeart Valve Disease: State of the ArtJose ZamoranoОценок пока нет
- Porto Biomedical JournalДокумент7 страницPorto Biomedical JournalzzakieОценок пока нет
- Agis Mira Dewi, S.kedДокумент35 страницAgis Mira Dewi, S.kedAgiish EMdeОценок пока нет
- Type 2 diabetes and periodontal diseaseДокумент10 страницType 2 diabetes and periodontal diseaseObed AZARD -Оценок пока нет
- Assesment GOДокумент17 страницAssesment GOBHUENDOCRINE SRОценок пока нет
- Treating Gout and Lowering Uric Acid LevelsДокумент10 страницTreating Gout and Lowering Uric Acid LevelsMelvri BisaiОценок пока нет
- Gouty ArthritisДокумент12 страницGouty ArthritisManoj KandoiОценок пока нет
- RMC 152 VДокумент8 страницRMC 152 VJairo ChavezОценок пока нет
- Rareparotidgland Diseases: Akshay Sanan,, David M. CognettiДокумент12 страницRareparotidgland Diseases: Akshay Sanan,, David M. CognettiGiovanniAnggastaОценок пока нет
- CMS Int. Med1 AnswersДокумент15 страницCMS Int. Med1 AnswersDiego Al Gutierrez50% (2)
- Rheumatoid ArthritisДокумент7 страницRheumatoid ArthritisPrince OcsanОценок пока нет
- Thyroid Eye Disease: Autoimmune Disorder Characterised by Infiltrative OrbitopathyДокумент43 страницыThyroid Eye Disease: Autoimmune Disorder Characterised by Infiltrative OrbitopathyBIBI MOHANANОценок пока нет
- Urticaria: Evaluation and Treatment: Paul Schaefer, MD, PHD, University of Toledo College of Medicine, Toledo, OhioДокумент7 страницUrticaria: Evaluation and Treatment: Paul Schaefer, MD, PHD, University of Toledo College of Medicine, Toledo, OhiocorsaruОценок пока нет
- Concept Map in NursingДокумент3 страницыConcept Map in NursingMaish Kevin0% (1)
- Gout Cure: Banish your Gout for Good and Become Pain Free using Natural Home Remedies, Exercise and DietОт EverandGout Cure: Banish your Gout for Good and Become Pain Free using Natural Home Remedies, Exercise and DietОценок пока нет
- Glo Me Rulo NephritisДокумент19 страницGlo Me Rulo NephritisAshley HumphreyОценок пока нет
- JCM 10 01880 v2Документ15 страницJCM 10 01880 v2Tamara MuñozОценок пока нет
- Fundamentals of Rheumatoid Arthritis and Various Homoeopathic Trials in Patients of Rheumatoid Arthritis: An UpdateДокумент6 страницFundamentals of Rheumatoid Arthritis and Various Homoeopathic Trials in Patients of Rheumatoid Arthritis: An UpdateHomoeopathic PulseОценок пока нет
- GoutДокумент5 страницGoutDe Sesto Rhys Carlo100% (2)
- Laporan Data Mini ProjekДокумент6 страницLaporan Data Mini ProjekDebby ElviraОценок пока нет
- ALL Book PDFДокумент94 страницыALL Book PDFMutiana A KidiwОценок пока нет
- Preoperative Femoral Nerve Block in Hip ArthroscopДокумент2 страницыPreoperative Femoral Nerve Block in Hip ArthroscopDebby ElviraОценок пока нет
- Ultrasound Guided Femoral Nerve BlockДокумент10 страницUltrasound Guided Femoral Nerve BlockDebby ElviraОценок пока нет
- Prevention and Management of Gastro Varices and HemorrhageДокумент17 страницPrevention and Management of Gastro Varices and HemorrhageBegnailson RibeiroОценок пока нет
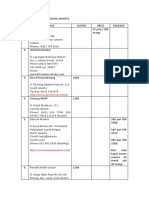
- Outdoor Wedding Venues in JakartaДокумент2 страницыOutdoor Wedding Venues in JakartaDebby ElviraОценок пока нет
- All About Vaginal DischargeДокумент1 страницаAll About Vaginal DischargeDebby ElviraОценок пока нет
- Femoral Nerve Block GuideДокумент7 страницFemoral Nerve Block GuideDebby ElviraОценок пока нет
- Femoral Block AnesthesiaДокумент4 страницыFemoral Block AnesthesiaDebby ElviraОценок пока нет
- Burn InjuryДокумент1 страницаBurn InjuryDebby ElviraОценок пока нет
- Wedding Planner PrintableДокумент2 страницыWedding Planner PrintableDebby ElviraОценок пока нет
- Burn InjuryДокумент1 страницаBurn InjuryDebby ElviraОценок пока нет
- A New Species of Zingiber (Zingiberaceae) From Lao P.D.RДокумент6 страницA New Species of Zingiber (Zingiberaceae) From Lao P.D.RDebby ElviraОценок пока нет
- Bab 154 Anemia Pada Penyakit Kronik PDFДокумент2 страницыBab 154 Anemia Pada Penyakit Kronik PDFDebby ElviraОценок пока нет
- Kdigo 2012 CKD GLДокумент163 страницыKdigo 2012 CKD GLOkky Sari Rahayu100% (1)
- RHD - Diagnosis&management - Oct 2008Документ21 страницаRHD - Diagnosis&management - Oct 2008annisazafiraОценок пока нет
- Baby Massage Consultation Form - November 2017Документ1 страницаBaby Massage Consultation Form - November 2017api-257327106Оценок пока нет
- PracticeWise Blue Menu of Evidence-Based InterventionsДокумент5 страницPracticeWise Blue Menu of Evidence-Based InterventionsLem BoneteОценок пока нет
- Review On Surge Drug Delivery TechnologyДокумент8 страницReview On Surge Drug Delivery TechnologyNayeli MercadoОценок пока нет
- Gout and Hyperuricemia: PathophysiologyДокумент1 страницаGout and Hyperuricemia: Pathophysiologyسمرة طايبОценок пока нет
- Thoughts Thoughts: 'Universe, Please Help Me Maintain An Effective Meditative-State. Thank You.'Документ4 страницыThoughts Thoughts: 'Universe, Please Help Me Maintain An Effective Meditative-State. Thank You.'Mincheol KangОценок пока нет
- Child AbuseДокумент5 страницChild AbusePeng Peng LimОценок пока нет
- Leptin HormoneДокумент21 страницаLeptin Hormonemarah almahameed100% (2)
- Jack Poylangada - Copy of Stamper Self-Care JournalДокумент8 страницJack Poylangada - Copy of Stamper Self-Care Journalapi-503633296100% (3)
- Nurs 205 Concept MapДокумент1 страницаNurs 205 Concept MapJami SpearsОценок пока нет
- Wound Healing SchwartzДокумент37 страницWound Healing SchwartzCarla Putri Chandra100% (1)
- English Iii: University of Guayaquil Facultad Piloto de OdontologíaДокумент4 страницыEnglish Iii: University of Guayaquil Facultad Piloto de OdontologíaDianitaVelezPincayОценок пока нет
- Congenital Syphilis Causes and TreatmentДокумент4 страницыCongenital Syphilis Causes and TreatmentAlya Putri Khairani100% (1)
- Pharmaceutical ExipientДокумент14 страницPharmaceutical ExipientShekhar SinghОценок пока нет
- Jeff Green Chiron Through The SignsДокумент7 страницJeff Green Chiron Through The Signsjasminschade8322100% (15)
- Jurnal 1 - Family Counseling in Malaysia Current Issues and PracticesДокумент7 страницJurnal 1 - Family Counseling in Malaysia Current Issues and PracticesMazlan D'GreatОценок пока нет
- Dysfunctional Gastrointestinal Motility Maybe Related To Sedentary Lifestyle and Limited Water Intake As Evidenced byДокумент6 страницDysfunctional Gastrointestinal Motility Maybe Related To Sedentary Lifestyle and Limited Water Intake As Evidenced byCecil MonteroОценок пока нет
- Surgical Approaches To The Skull BaseДокумент2 страницыSurgical Approaches To The Skull Baseİbrahim ErkutluОценок пока нет
- End of Life ManualДокумент238 страницEnd of Life ManualJeffery TaylorОценок пока нет
- Fact Sheet Squamous Cell Carcinoma Oct 2013Документ10 страницFact Sheet Squamous Cell Carcinoma Oct 2013Triven Nair HutabaratОценок пока нет
- Drugs in PregnancyДокумент14 страницDrugs in Pregnancyhenry_poirotОценок пока нет
- Psychology of Al-GhazaliДокумент48 страницPsychology of Al-GhazaliZainudin IsmailОценок пока нет
- Repertory: Information On Health Concerns in A Health DirectoryДокумент17 страницRepertory: Information On Health Concerns in A Health DirectoryShalinta Dubey SharmaОценок пока нет
- Bmet 262 Outline 2022 2023Документ12 страницBmet 262 Outline 2022 2023Emmanuel PrahОценок пока нет
- Client Intake FormsДокумент5 страницClient Intake FormsGuillaume VingtcentОценок пока нет
- Aromatherapy PRДокумент1 страницаAromatherapy PRNilamdeen Mohamed ZamilОценок пока нет
- Final Past Papers With Common MCQS: MedicineДокумент17 страницFinal Past Papers With Common MCQS: MedicineKasun PereraОценок пока нет
- Nada Lincomycyn and Espectynomycin Solubleucm061812Документ4 страницыNada Lincomycyn and Espectynomycin Solubleucm061812laurz95Оценок пока нет
- Grade9 STE Con.-Chem. Q4 Module-5 Wk6 ADMДокумент20 страницGrade9 STE Con.-Chem. Q4 Module-5 Wk6 ADMChelzy CatabasОценок пока нет
- COE WorksheetДокумент16 страницCOE WorksheetiloveraynaОценок пока нет
- Mental health test questionsДокумент5 страницMental health test questionsclarheenaОценок пока нет