Вам также может понравиться
- Gender Quest WorkbookДокумент191 страницаGender Quest WorkbookMichaella Ryan Quinn0% (3)
- Male Infertility, Diagnosis and Recent ManagementДокумент77 страницMale Infertility, Diagnosis and Recent ManagementDR SHASHWAT JANIОценок пока нет
- AmenorrheaДокумент41 страницаAmenorrheaBonitavanyОценок пока нет
- GENDER and SOCIETYДокумент42 страницыGENDER and SOCIETYlachimolala. kookieee97Оценок пока нет
- Module Mol Chapter 7Документ78 страницModule Mol Chapter 7eyoelОценок пока нет
- Identification and Management of Ambiguous GenitaliaДокумент31 страницаIdentification and Management of Ambiguous Genitaliateslimolakunleraji100% (1)
- Sex Chromosomes and Sex DeterminationДокумент22 страницыSex Chromosomes and Sex DeterminationJeru Bisnar ClementeОценок пока нет
- Compare and Contrast Process in Plants and Animals: Reproduction and DevelopmentДокумент64 страницыCompare and Contrast Process in Plants and Animals: Reproduction and DevelopmentMarites PacañaОценок пока нет
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyОт EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyОценок пока нет
- Gender and Society 1-3Документ20 страницGender and Society 1-3Zed Deguzman100% (4)
- Male Infertility 2018 PDFДокумент47 страницMale Infertility 2018 PDFasshyriaОценок пока нет
- Ima Jamnagar Directory 2014Документ32 страницыIma Jamnagar Directory 2014DR.MAULIK SHAH67% (3)
- Neonatal Skin CareДокумент40 страницNeonatal Skin CareDR.MAULIK SHAH67% (3)
- 26.7.16-Approach To Ambiguous Genitalia - Is It A Boy or Girl PDFДокумент57 страниц26.7.16-Approach To Ambiguous Genitalia - Is It A Boy or Girl PDFBlueash BehОценок пока нет
- Disorder of Determination and Sex DifferentiationДокумент62 страницыDisorder of Determination and Sex DifferentiationSYAFIRA INAYAHОценок пока нет
- AmenorrheaДокумент56 страницAmenorrheaMrTriumphantОценок пока нет
- 56 Ambiguous GenitaliaДокумент8 страниц56 Ambiguous GenitalianasibdinОценок пока нет
- Intersex & Ambigous GenitaliaДокумент46 страницIntersex & Ambigous Genitaliahayssam rashwanОценок пока нет
- 17-Mrdi DLP-1Документ114 страниц17-Mrdi DLP-1Jawad Ul HaqОценок пока нет
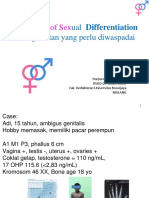
- Disorders of Sexual Differentiation: A Amirhakimi, MD Pediatric Endocrinologist Shiraz University of Medical SciencesДокумент30 страницDisorders of Sexual Differentiation: A Amirhakimi, MD Pediatric Endocrinologist Shiraz University of Medical SciencesTitus RheinhardoОценок пока нет
- IntersexnnДокумент66 страницIntersexnnSyahputraWibowoОценок пока нет
- Male Infertility Omer Onur CakirДокумент35 страницMale Infertility Omer Onur CakirLakshay GulatiОценок пока нет
- 01 Disorders of Sexual DevelopmentДокумент29 страниц01 Disorders of Sexual DevelopmentAbeer SarayraОценок пока нет
- Tom DeMarkДокумент41 страницаTom DeMarktoughnedglassОценок пока нет
- Cryptorchidism: Discussion Barasa Moses (Med VI)Документ30 страницCryptorchidism: Discussion Barasa Moses (Med VI)Moses BarasaОценок пока нет
- Primary AmenorrheaДокумент33 страницыPrimary AmenorrheaZaraОценок пока нет
- What Comes Under The DSD Umbrella?Документ50 страницWhat Comes Under The DSD Umbrella?Scott LoveОценок пока нет
- 29 Ian DSD. PubertateaДокумент64 страницы29 Ian DSD. Pubertateaadelinamihaela7Оценок пока нет
- Ambiguous GenitaliaДокумент16 страницAmbiguous Genitaliamohdmaghyreh100% (1)
- Disorders of Sexual DevelopmentpptДокумент51 страницаDisorders of Sexual Developmentpptwende kassahunОценок пока нет
- Anomalii Ale Diferentierii SexualeДокумент43 страницыAnomalii Ale Diferentierii SexualeAlexandru Dan ArseneОценок пока нет
- 4 GeneticsДокумент27 страниц4 GeneticszahuuОценок пока нет
- 09-28-15 CAH Grand RoundsДокумент55 страниц09-28-15 CAH Grand Roundsnila sari batubaraОценок пока нет
- Obstetrics & Gynecology: Original Review & Revision HyderabadДокумент739 страницObstetrics & Gynecology: Original Review & Revision Hyderabad24k.avinashОценок пока нет
- Sexuality and IntersexualityДокумент23 страницыSexuality and IntersexualityManu BharadwazОценок пока нет
- 2021 HID Repro Unit Recap 1 - FinalДокумент63 страницы2021 HID Repro Unit Recap 1 - Finalf3er3Оценок пока нет
- Genetika ManusiaДокумент35 страницGenetika ManusiaWndy 0903Оценок пока нет
- Ambiguous Genitalia (Disorders of Sexual Differentiation) : DR GwerДокумент18 страницAmbiguous Genitalia (Disorders of Sexual Differentiation) : DR GwerMalueth AnguiОценок пока нет
- Amen or RheaДокумент41 страницаAmen or Rheakhadzx100% (2)
- 37 UPDATED Genetic+Diseases Allen PDFДокумент36 страниц37 UPDATED Genetic+Diseases Allen PDFSuh DudeОценок пока нет
- Sexual Differentiation Anomalies+Puberty - PPT Fara PozeДокумент49 страницSexual Differentiation Anomalies+Puberty - PPT Fara PozeAmira AsaadОценок пока нет
- Cryptorchidism: - 4 Fold Higher Than Average RiskДокумент52 страницыCryptorchidism: - 4 Fold Higher Than Average RiskRidwan Hadinata SalimОценок пока нет
- MEETING 6 AmenorrheaДокумент41 страницаMEETING 6 AmenorrheaNader KhouryОценок пока нет
- Amenorrheamadeeasyslideshare 2015 150423165553 Conversion Gate01 PDFДокумент51 страницаAmenorrheamadeeasyslideshare 2015 150423165553 Conversion Gate01 PDFHerman FiraОценок пока нет
- Ambiguousgenitalia 150621055259 Lva1 App6891Документ66 страницAmbiguousgenitalia 150621055259 Lva1 App6891imnetuyОценок пока нет
- Disorders of Sexual DevelopmentДокумент19 страницDisorders of Sexual DevelopmentJoanne May100% (1)
- 0127「小兒遺傳及代謝」講師陳燕彰醫師Документ114 страниц0127「小兒遺傳及代謝」講師陳燕彰醫師許懷朔Оценок пока нет
- Disoreder Sex of DevelopmentДокумент37 страницDisoreder Sex of DevelopmentBesth To Frynce HutabaratОценок пока нет
- Disorders of Gonadal and Sexual Development: BESHG Postgraduate Course in Human GeneticsДокумент43 страницыDisorders of Gonadal and Sexual Development: BESHG Postgraduate Course in Human GeneticsDarmawan HariyantoОценок пока нет
- Infertility: by Kenbon SДокумент58 страницInfertility: by Kenbon SgimОценок пока нет
- Mission Fmge Obg Day-6 - 231114 - 215211Документ137 страницMission Fmge Obg Day-6 - 231114 - 215211CastleKGОценок пока нет
- 2 AmenorrheaДокумент41 страница2 AmenorrheaKilp MosesОценок пока нет
- Kasus Istimewa - Amenorrhea PrimerДокумент45 страницKasus Istimewa - Amenorrhea PrimerMuhammad SukriОценок пока нет
- Sexdifferentiation1 151124152908 Lva1 App6891Документ17 страницSexdifferentiation1 151124152908 Lva1 App6891BeatrizEguilosAspirasОценок пока нет
- Ambiguous Genitalia2Документ27 страницAmbiguous Genitalia2Islam AminОценок пока нет
- DSD Harjoedi Pedendo 19Документ42 страницыDSD Harjoedi Pedendo 19bolabundarОценок пока нет
- Dr. Bassem W. Yani, MD Diploma of Urology, FEBU, FCS, Cairo, EGYPT Consultant Urologist Uth Lusaka ZambiaДокумент43 страницыDr. Bassem W. Yani, MD Diploma of Urology, FEBU, FCS, Cairo, EGYPT Consultant Urologist Uth Lusaka ZambiaMohammed AadeelОценок пока нет
- Developmental Biology XL 138: Week 10Документ61 страницаDevelopmental Biology XL 138: Week 10Soji AdimulaОценок пока нет
- Male InfertilityДокумент14 страницMale InfertilityDavid TurnerОценок пока нет
- Precocious PubertyДокумент4 страницыPrecocious PubertyHa Jae kyeongОценок пока нет
- Puberty (OBGYN Presentation #1)Документ15 страницPuberty (OBGYN Presentation #1)Alex KadirОценок пока нет
- Disorders of Sexual DevelopmentДокумент48 страницDisorders of Sexual DevelopmentTofitofi TofiОценок пока нет
- Evaluation of Infertile CoupleДокумент28 страницEvaluation of Infertile CoupleSanvi shrimaliОценок пока нет
- Androgen Insensitivity Syndrome (Ais)Документ18 страницAndrogen Insensitivity Syndrome (Ais)Junbek nov23Оценок пока нет
- Cryptorchidism (Undescended Testes)Документ22 страницыCryptorchidism (Undescended Testes)shreerama nairОценок пока нет
- Patho of Male Repro. Sys. & STD: Azrina Zainal AbidinДокумент58 страницPatho of Male Repro. Sys. & STD: Azrina Zainal Abidinﻧﻮﺭﻭﻝ ﻋﻠﻴﻨﺎ ﺣﺎﺝ يهيОценок пока нет
- IMA Press Release Antibiotics - 31.7.2014Документ4 страницыIMA Press Release Antibiotics - 31.7.2014DR.MAULIK SHAHОценок пока нет
- IMA - CIRCULAR Felicitation 2014Документ2 страницыIMA - CIRCULAR Felicitation 2014DR.MAULIK SHAHОценок пока нет
- Chiranjeevi & Balskaha WorkshopДокумент1 страницаChiranjeevi & Balskaha WorkshopDR.MAULIK SHAHОценок пока нет
- List of Children For FelicitationДокумент3 страницыList of Children For FelicitationDR.MAULIK SHAHОценок пока нет
- FORM Felicitation 2014 PDFДокумент1 страницаFORM Felicitation 2014 PDFDR.MAULIK SHAHОценок пока нет
- C.M. Setu YojnaДокумент8 страницC.M. Setu YojnaDR.MAULIK SHAH50% (2)
- Gujarat State Law On 'Assault On Doctors'Документ9 страницGujarat State Law On 'Assault On Doctors'DR.MAULIK SHAHОценок пока нет
- Registration FormДокумент1 страницаRegistration FormDR.MAULIK SHAHОценок пока нет
- Ima, Jamnagar Branch Directory FormДокумент1 страницаIma, Jamnagar Branch Directory FormDR.MAULIK SHAHОценок пока нет
- Fluid & Elecrolytes Management in NewbornsДокумент42 страницыFluid & Elecrolytes Management in NewbornsDR.MAULIK SHAHОценок пока нет
- Kangaroo Mother CareДокумент23 страницыKangaroo Mother CareDR.MAULIK SHAH100% (2)
- Late Life DepressionДокумент27 страницLate Life DepressionDR.MAULIK SHAHОценок пока нет
- HINDI-Novel H1 N1 Influenza PandemicДокумент30 страницHINDI-Novel H1 N1 Influenza PandemicDR.MAULIK SHAHОценок пока нет
- Changing Trends-Pediatric Maintenance IV FluidДокумент21 страницаChanging Trends-Pediatric Maintenance IV FluidDR.MAULIK SHAHОценок пока нет
- The Making of 'RAVANA'Документ10 страницThe Making of 'RAVANA'DR.MAULIK SHAHОценок пока нет
- Kangaroo Mother CareДокумент23 страницыKangaroo Mother CareDR.MAULIK SHAH100% (2)
- New Born Baby WardДокумент19 страницNew Born Baby WardDR.MAULIK SHAHОценок пока нет
- Swine Flu (H1N1) Informative PostersДокумент3 страницыSwine Flu (H1N1) Informative PostersDR.MAULIK SHAH100% (1)
- Chromosomal MutationДокумент7 страницChromosomal Mutationchastine daneОценок пока нет
- Drosophila Lab Write UpДокумент13 страницDrosophila Lab Write Upapi-585837255Оценок пока нет
- LAS in Health 8 Quarter 1Документ6 страницLAS in Health 8 Quarter 1Rovilyn Dizon100% (1)
- Gas Module 1 PDFДокумент58 страницGas Module 1 PDFHIEZEL BAYUGОценок пока нет
- Genetics Essentials Concepts and Connections 3rd Edition Pierce Test Bank 1Документ36 страницGenetics Essentials Concepts and Connections 3rd Edition Pierce Test Bank 1hollyclarkebfaoejwrny100% (25)
- Case Study Sry Not SryДокумент13 страницCase Study Sry Not Sryapi-357511225Оценок пока нет
- Module 2 Gender and Society Week 2 Gender and SexualityДокумент7 страницModule 2 Gender and Society Week 2 Gender and SexualityKougane SanОценок пока нет
- Class X Diwali Holiday AssignmentДокумент47 страницClass X Diwali Holiday AssignmentKunal SahuОценок пока нет
- Lesson 1 - Sex and GenderДокумент5 страницLesson 1 - Sex and Genderweyn feitОценок пока нет
- Sex Ambigus DR Bambang TridjajaДокумент43 страницыSex Ambigus DR Bambang TridjajaAdjie PreetОценок пока нет
- In RabbitsДокумент8 страницIn Rabbitsjay bordenОценок пока нет
- Gender DysphoriaДокумент13 страницGender DysphoriaKarla DreamsОценок пока нет
- Test Bank For Gender Ideas Interactions Institutions 2nd by WadeДокумент8 страницTest Bank For Gender Ideas Interactions Institutions 2nd by WadeAshley Piper100% (24)
- Sex Ratio DistortionДокумент17 страницSex Ratio DistortionAdam ZHUОценок пока нет
- Turner Syndrome: A Guide For FamiliesДокумент30 страницTurner Syndrome: A Guide For FamiliesTatiana Pogo RamosОценок пока нет
- Legal and Political Framework On GenderДокумент6 страницLegal and Political Framework On GenderJoe Brayle JoeyОценок пока нет
- Gen Chapter Summary 5Документ15 страницGen Chapter Summary 5Bismarck John SalazarОценок пока нет
- Module 1: Introduction To Gender PsychologyДокумент12 страницModule 1: Introduction To Gender PsychologyTwisha SaxenaОценок пока нет
- 2nd Term Biology Ss3Документ20 страниц2nd Term Biology Ss3Wisdom Lawal (Wizywise)Оценок пока нет
- Ppt. Sex LinkageДокумент38 страницPpt. Sex LinkageAj Myco EstorОценок пока нет
- Villanueva - Cleo - Mel - Sex ChromosomesДокумент6 страницVillanueva - Cleo - Mel - Sex ChromosomesCleo VillanuevaОценок пока нет
- Sex Determination MechanismsДокумент31 страницаSex Determination MechanismsZara HussainОценок пока нет
- (Eng) Sex and Gender - David NewtonДокумент356 страниц(Eng) Sex and Gender - David Newtondaon bawangОценок пока нет
- Bio 511 c4Документ88 страницBio 511 c4Athirah JeffryОценок пока нет