Вам также может понравиться
- Ob b9c7f6 l4000 Uk Tweaking TipsДокумент11 страницOb b9c7f6 l4000 Uk Tweaking TipsAlfonsobcnОценок пока нет
- Sailmaker GuidebookДокумент31 страницаSailmaker GuidebookAlfonsobcnОценок пока нет
- 2013 NorthSails SailTrimДокумент60 страниц2013 NorthSails SailTrimAlfonsobcn100% (6)
- Splice BookДокумент30 страницSplice BooklmantuanoОценок пока нет
- 2013 NorthSails SailTrimДокумент60 страниц2013 NorthSails SailTrimAlfonsobcn100% (6)
- Windsurfing Manual: Hoofer Sailing ClubДокумент30 страницWindsurfing Manual: Hoofer Sailing ClubAlfonsobcnОценок пока нет
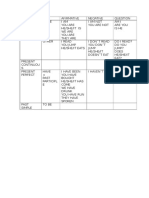
- English VerbsДокумент1 страницаEnglish VerbsAlfonsobcnОценок пока нет
- Locked AwayДокумент5 страницLocked AwayAlfonsobcnОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- IFU 1110004905 Fastep DEN-W23M(2滴buffer)(C-T1-T2线)CE 英文说明书 Polymed地址(彩色A4双面双胶)1张Документ2 страницыIFU 1110004905 Fastep DEN-W23M(2滴buffer)(C-T1-T2线)CE 英文说明书 Polymed地址(彩色A4双面双胶)1张BPG ServiceОценок пока нет
- Med Surg Chap QuestionsДокумент9 страницMed Surg Chap Questionslani0% (1)
- Proof of Safety Robert Tisserand PDFДокумент22 страницыProof of Safety Robert Tisserand PDFMahu Pessoa100% (2)
- Drill 15 16 Exposition AnalyticalДокумент5 страницDrill 15 16 Exposition AnalyticaliqsaneОценок пока нет
- Effectiveness of Garlic (Allium Sativum) As Antimicrobial Agent Against Bacteria Causing Urinary Tract InfectionДокумент4 страницыEffectiveness of Garlic (Allium Sativum) As Antimicrobial Agent Against Bacteria Causing Urinary Tract InfectionSabrina JonesОценок пока нет
- Hand Hygiene Self Assessment FrameworkДокумент9 страницHand Hygiene Self Assessment FrameworkWiDya EmiLiaОценок пока нет
- Blood Agar Base (Infusion Agar) : Intended Use Summary and ExplanationДокумент2 страницыBlood Agar Base (Infusion Agar) : Intended Use Summary and ExplanationSarehElizabetОценок пока нет
- Medical Surgical NursingДокумент38 страницMedical Surgical NursingTripti PunОценок пока нет
- CogwheelДокумент4 страницыCogwheelRimsha RanaОценок пока нет
- Vol. 2 No. 10Документ58 страницVol. 2 No. 10Lindsey RobbinsОценок пока нет
- Dengue Clinical Presentation - History, Physical ExaminationДокумент6 страницDengue Clinical Presentation - History, Physical Examinationm.m.m.mОценок пока нет
- Rabipur - (EMC) Print FriendlyДокумент8 страницRabipur - (EMC) Print Friendlyshreyas_chandor3802Оценок пока нет
- Seri Final NotesДокумент179 страницSeri Final Notesbharath gowdaОценок пока нет
- First Aid NotesДокумент6 страницFirst Aid NotesDivya DhashiniОценок пока нет
- Urine Albumin NewДокумент10 страницUrine Albumin NewPriya Sharma100% (1)
- Update on Lower Lid Blepharoplasty TechniquesДокумент23 страницыUpdate on Lower Lid Blepharoplasty TechniquesNur baitiОценок пока нет
- Essay On AidsДокумент6 страницEssay On AidsBharat SinghОценок пока нет
- Aortic ValveДокумент8 страницAortic ValveIfeanyichukwu OgbonnayaОценок пока нет
- Liver Abscess Diagnosis and TreatmentДокумент12 страницLiver Abscess Diagnosis and TreatmentSimon Messi SiringoringoОценок пока нет
- Cardiac MedicationsДокумент8 страницCardiac Medicationsangeline totaram100% (2)
- Heinz Kohut - Self PsychologyДокумент49 страницHeinz Kohut - Self PsychologyDesiree Pescasio DimasuayОценок пока нет
- 7 Vs 14days Gram Negative SepsisДокумент8 страниц7 Vs 14days Gram Negative SepsisPavan KumarОценок пока нет
- Detoxification of Pesticide Waste Via Activated Carbon Adsorption ProcessДокумент11 страницDetoxification of Pesticide Waste Via Activated Carbon Adsorption ProcessNadia MandasariОценок пока нет
- Pol TakesДокумент84 страницыPol Takesfauzi jayaОценок пока нет
- Hot and Cold Application - PPTX RevisedДокумент61 страницаHot and Cold Application - PPTX RevisedMicah HuanОценок пока нет
- 2 02-Electrocardiography PDFДокумент17 страниц2 02-Electrocardiography PDFMiguel DomingoОценок пока нет
- Setting up MRI Scan CentresДокумент86 страницSetting up MRI Scan CentresGokilavani RajagopalОценок пока нет
- The New Super Nutrient Food - Raw Banana FlourДокумент5 страницThe New Super Nutrient Food - Raw Banana FlourSandeep Goud kolalaОценок пока нет
- Mendelian Genetics - Test #2 ReviewДокумент6 страницMendelian Genetics - Test #2 Reviewfalefalk123Оценок пока нет
- Davao Doctors College nursing program drug study for ranitidineДокумент4 страницыDavao Doctors College nursing program drug study for ranitidinePao LaurenteОценок пока нет