Вам также может понравиться
- 2 Hipaa Front Notices-Page 1 2-13Документ1 страница2 Hipaa Front Notices-Page 1 2-13api-214017719Оценок пока нет
- HIPAA Privacy Authorization Form: 2835 20 Street Vero Beach, FL 32960 Telephone: (772) 299-3003 Fax: (772) 299-3005Документ3 страницыHIPAA Privacy Authorization Form: 2835 20 Street Vero Beach, FL 32960 Telephone: (772) 299-3003 Fax: (772) 299-3005api-104636361Оценок пока нет
- Psycho Social AssessmentДокумент10 страницPsycho Social Assessmentaa985rocketmailОценок пока нет
- Records ReleaseДокумент1 страницаRecords ReleaseChad MartinОценок пока нет
- Hmc621 Special Auth To Release InfoДокумент1 страницаHmc621 Special Auth To Release InfoJonathan SchmidtОценок пока нет
- HIPAA authorization formДокумент3 страницыHIPAA authorization formSalsabilla NurfaniaОценок пока нет
- Standard Authorization FormДокумент3 страницыStandard Authorization FormedzuckermanОценок пока нет
- CGH Release of InformationДокумент2 страницыCGH Release of InformationEnoy LuОценок пока нет
- Florida Designation of Health Surrogate - BlankДокумент1 страницаFlorida Designation of Health Surrogate - BlankJesco IvoryОценок пока нет
- Release of InformationДокумент2 страницыRelease of Informationxstn15Оценок пока нет
- New Patient Reg FormДокумент7 страницNew Patient Reg FormDr.HunanyanОценок пока нет
- JIT 2363 Authorization To Release Med RecordsДокумент2 страницыJIT 2363 Authorization To Release Med Recordsalan benedettaОценок пока нет
- JMPN Health Information DisclosureДокумент2 страницыJMPN Health Information DisclosureTadilakshmikiranОценок пока нет
- Adult Intake-1Документ13 страницAdult Intake-1Kimberly StanfordОценок пока нет
- W A M R P ?: HAT RE Y Ights As A ArticipantДокумент3 страницыW A M R P ?: HAT RE Y Ights As A ArticipantJack TedescoОценок пока нет
- Hipaa Authorization For Use or Disclosure of Health InformationДокумент3 страницыHipaa Authorization For Use or Disclosure of Health InformationNigil josephОценок пока нет
- CFLPRIVACYДокумент1 страницаCFLPRIVACYLoriОценок пока нет
- Authorization To Disclose Medical InformationДокумент2 страницыAuthorization To Disclose Medical InformationFindLegalFormsОценок пока нет
- Mark Wesley Joseph SmithДокумент2 страницыMark Wesley Joseph SmithMohammedОценок пока нет
- Roi Authorization Revision Final 08 27 13 PDFДокумент1 страницаRoi Authorization Revision Final 08 27 13 PDFHenry PannellОценок пока нет
- 641 Request Amendment of Your PHIДокумент3 страницы641 Request Amendment of Your PHIedzuckermanОценок пока нет
- Innacle: Authorization To Receive or Release Medical InformationДокумент2 страницыInnacle: Authorization To Receive or Release Medical InformationFrank ZОценок пока нет
- Hipaa Privacy3 09Документ3 страницыHipaa Privacy3 09Jennifer WalkerОценок пока нет
- TUE - WADA Version 2016-EnДокумент4 страницыTUE - WADA Version 2016-EnYannick MOSSUSОценок пока нет
- KP Records Release FormДокумент3 страницыKP Records Release FormKellyОценок пока нет
- Healthy LIC - Patient CONSENT Form EnglishДокумент4 страницыHealthy LIC - Patient CONSENT Form EnglishTheFloatingHospitalОценок пока нет
- Template of TUE Application FormДокумент4 страницыTemplate of TUE Application FormWilsfunОценок пока нет
- Advocare Consent Disclosure Authorization PDFДокумент2 страницыAdvocare Consent Disclosure Authorization PDFAsnaifa Bint MamintalОценок пока нет
- Regional Paramedical Services, Inc.Документ1 страницаRegional Paramedical Services, Inc.Richard SheddОценок пока нет
- Attending Physician's Statement for Death ClaimДокумент2 страницыAttending Physician's Statement for Death ClaimKen CelesteОценок пока нет
- Andy Anderson, M.A., PLPC 2850 West Clay, Suite 255 Saint Charles, MO 63301 Phone: (636) 699-0872 FAX: (636) 625-0839Документ1 страницаAndy Anderson, M.A., PLPC 2850 West Clay, Suite 255 Saint Charles, MO 63301 Phone: (636) 699-0872 FAX: (636) 625-0839api-55970082Оценок пока нет
- Privacy AcknowledgementДокумент1 страницаPrivacy Acknowledgementharrisk31Оценок пока нет
- Authorization For Release and Disclosure For SCDC Medical Records 2019Документ1 страницаAuthorization For Release and Disclosure For SCDC Medical Records 2019Sara SnowОценок пока нет
- HIPAA Release FormДокумент3 страницыHIPAA Release FormBecky King FennerОценок пока нет
- Patient Intake and Consent FormsДокумент13 страницPatient Intake and Consent FormsSam EmekaОценок пока нет
- Credential IngДокумент13 страницCredential Ingdr_rajatjainОценок пока нет
- Immmunization FormДокумент1 страницаImmmunization Formnarutokun0Оценок пока нет
- Med Records Release FROM HOTVДокумент1 страницаMed Records Release FROM HOTVHeart of the Valley, Pediatric CardiologyОценок пока нет
- Data Privacy Consent: II. Consent For Procedure(s)Документ1 страницаData Privacy Consent: II. Consent For Procedure(s)kОценок пока нет
- Notice of Privacy PracticesДокумент5 страницNotice of Privacy PracticesjirehcounselingОценок пока нет
- Release FormДокумент1 страницаRelease FormRichard Dunn IIОценок пока нет
- Designation of Health Care Surrogate: Under 765.202, Florida StatutesДокумент2 страницыDesignation of Health Care Surrogate: Under 765.202, Florida StatutesClari HerreraОценок пока нет
- Medical Consent Form For BabysitterДокумент2 страницыMedical Consent Form For BabysitterSalman KhatriОценок пока нет
- Hipaa 1Документ1 страницаHipaa 1Gregory KnispelОценок пока нет
- Hipaa Journal Hipaa Release Form v1Документ3 страницыHipaa Journal Hipaa Release Form v1pialee royОценок пока нет
- HEALTH CARE POWER OF ATTORNEY (SC Statutory Form)Документ7 страницHEALTH CARE POWER OF ATTORNEY (SC Statutory Form)Alexandria Broughton SkinnerОценок пока нет
- Informed Consent For Testing Rev-Oct 2019Документ1 страницаInformed Consent For Testing Rev-Oct 2019KatieОценок пока нет
- AUTHORIZATION FOR MEDICAL RECORDSДокумент1 страницаAUTHORIZATION FOR MEDICAL RECORDSlostindallasОценок пока нет
- Affidavit - Religious Exemption - AdultДокумент2 страницыAffidavit - Religious Exemption - AdultSandra GonzalezОценок пока нет
- Acuse de Recibo 03Документ1 страницаAcuse de Recibo 03KATYA VARGASОценок пока нет
- Peace Corps Eating Disorder Treatment Summary Form PC-262-8 (Initial Approval 08/2012Документ4 страницыPeace Corps Eating Disorder Treatment Summary Form PC-262-8 (Initial Approval 08/2012Accessible Journal Media: Peace Corps DocumentsОценок пока нет
- Public Servant's QuestionnaireДокумент3 страницыPublic Servant's Questionnairegetsome100% (2)
- Medicaid AppealДокумент15 страницMedicaid Appealmtp7389Оценок пока нет
- Sample HIE Consent 2020 Update FinalДокумент1 страницаSample HIE Consent 2020 Update FinalKevin G. DavisОценок пока нет
- Patient Registration Form 13Документ4 страницыPatient Registration Form 13windawaty humolaОценок пока нет
- Authorization To Release Medical Records/InformationДокумент1 страницаAuthorization To Release Medical Records/InformationDeandra ChambersОценок пока нет
- Pursuant To The Health Insurance Portability and Accountability Act "HIPAA" of 4/14/03Документ1 страницаPursuant To The Health Insurance Portability and Accountability Act "HIPAA" of 4/14/03cmferrer2005Оценок пока нет
- Authorization For Release of Health Information Pursuant To HIPPA - New York299567420170403Документ2 страницыAuthorization For Release of Health Information Pursuant To HIPPA - New York299567420170403wsxОценок пока нет
- Cross-Training: The Medical Assistant WorkbookОт EverandCross-Training: The Medical Assistant WorkbookОценок пока нет
- 960 Email Confidentiality NoticesДокумент2 страницы960 Email Confidentiality NoticesedzuckermanОценок пока нет
- 641 Request Amendment of Your PHIДокумент1 страница641 Request Amendment of Your PHIedzuckermanОценок пока нет
- 1050 Feedback FormДокумент1 страница1050 Feedback FormedzuckermanОценок пока нет
- 960 Email Confidentiality NoticesДокумент1 страница960 Email Confidentiality NoticesedzuckermanОценок пока нет
- 631 Request Access To Your PHIДокумент1 страница631 Request Access To Your PHIedzuckermanОценок пока нет
- 653 Request An Accounting of DisclosuresДокумент1 страница653 Request An Accounting of DisclosuresedzuckermanОценок пока нет
- 661 Complaint FormДокумент1 страница661 Complaint FormedzuckermanОценок пока нет
- 800 HIPAA Policy & Procedures ManualДокумент7 страниц800 HIPAA Policy & Procedures ManualedzuckermanОценок пока нет
- 800 HIPAA Policy & Procedures ManualДокумент26 страниц800 HIPAA Policy & Procedures ManualedzuckermanОценок пока нет
- Request Form for Accounting of PHI DisclosuresДокумент1 страницаRequest Form for Accounting of PHI DisclosuresedzuckermanОценок пока нет
- 654 Form For An Accounting of DisclosuresДокумент1 страница654 Form For An Accounting of DisclosuresedzuckermanОценок пока нет
- 621 Request Alternative CommunicationДокумент1 страница621 Request Alternative CommunicationedzuckermanОценок пока нет
- 661 Complaint FormДокумент2 страницы661 Complaint FormedzuckermanОценок пока нет
- 654 Form For An Accounting of DisclosuresДокумент3 страницы654 Form For An Accounting of DisclosuresedzuckermanОценок пока нет
- 651 Medical Record Disclosures LogДокумент1 страница651 Medical Record Disclosures LogedzuckermanОценок пока нет
- 651 Medical Record Disclosures LogДокумент2 страницы651 Medical Record Disclosures LogedzuckermanОценок пока нет
- 490 Revoking and AuthorizationДокумент1 страница490 Revoking and AuthorizationedzuckermanОценок пока нет
- 621 Request Alternative CommunicationДокумент2 страницы621 Request Alternative CommunicationedzuckermanОценок пока нет
- 611 Request Limitations On CommunicationsДокумент2 страницы611 Request Limitations On CommunicationsedzuckermanОценок пока нет
- Revoke health info authorization formДокумент2 страницыRevoke health info authorization formedzuckermanОценок пока нет
- 641 Request Amendment of Your PHIДокумент3 страницы641 Request Amendment of Your PHIedzuckermanОценок пока нет
- 611 Request Limitations On CommunicationsДокумент1 страница611 Request Limitations On CommunicationsedzuckermanОценок пока нет
- 451 Standard Authorization FormДокумент1 страница451 Standard Authorization FormedzuckermanОценок пока нет
- Standard Authorization FormДокумент3 страницыStandard Authorization FormedzuckermanОценок пока нет
- 431 Consent To Use and DiscloseДокумент1 страница431 Consent To Use and DiscloseedzuckermanОценок пока нет
- 431 Consent To Use and DiscloseДокумент2 страницы431 Consent To Use and DiscloseedzuckermanОценок пока нет
- 412 The Briefer Notice of Privacy PracticesДокумент1 страница412 The Briefer Notice of Privacy PracticesedzuckermanОценок пока нет
- 411 Notice of Privacy Practices-LongДокумент3 страницы411 Notice of Privacy Practices-LongedzuckermanОценок пока нет
- 412 The Briefer Notice of Privacy PracticesДокумент3 страницы412 The Briefer Notice of Privacy PracticesedzuckermanОценок пока нет
- Carta Al Gobernador Rosselló Sobre El Ajuste Del Gobierno de Puerto Rico Incluido en El Plan Fiscal CertificadoДокумент5 страницCarta Al Gobernador Rosselló Sobre El Ajuste Del Gobierno de Puerto Rico Incluido en El Plan Fiscal CertificadoEmily RamosОценок пока нет
- 10 Day Workout Plan 260cf416 73ce 41ff b8f5 6b38f89aebc9Документ6 страниц10 Day Workout Plan 260cf416 73ce 41ff b8f5 6b38f89aebc9alexlucu21Оценок пока нет
- Badac AuditДокумент19 страницBadac AuditGeline BoreroОценок пока нет
- Management by ObjectivesДокумент16 страницManagement by Objectivespaminder100% (1)
- Misleading Headache Remedy Contained AcetanilideДокумент2 страницыMisleading Headache Remedy Contained AcetanilideSar CaermareОценок пока нет
- Patients Autonomy and Informed ConsentДокумент10 страницPatients Autonomy and Informed ConsentSandra GabasОценок пока нет
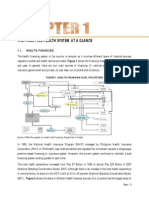
- Philippines health system overview: financing, facilities, human resourcesДокумент15 страницPhilippines health system overview: financing, facilities, human resourcesYL LYОценок пока нет
- Personal Financial Planning Case Study for Ahmad in 2013-2046Документ50 страницPersonal Financial Planning Case Study for Ahmad in 2013-2046Jahid Hasan100% (5)
- Express Scripts AnswerДокумент59 страницExpress Scripts AnswerjssherkowОценок пока нет
- McDermott-ltr To Veterans AffairsДокумент21 страницаMcDermott-ltr To Veterans AffairsAnna MooreОценок пока нет
- Lecture 2 The Australian Health System Health Systems and Economics PUBH5752Документ10 страницLecture 2 The Australian Health System Health Systems and Economics PUBH5752Mia MacMillanОценок пока нет
- Bier Vs BierДокумент1 страницаBier Vs BierwesleybooksОценок пока нет
- Deepakshi BillsДокумент4 страницыDeepakshi BillsC K ANANDОценок пока нет
- Uruguay Marijuana Legalization Law English TranslationДокумент20 страницUruguay Marijuana Legalization Law English Translationwebmaster@drugpolicy.orgОценок пока нет
- UAE Visa FormДокумент3 страницыUAE Visa Forma_mohid17100% (2)
- IndexofPublishResosandMCs1989 2018Документ24 страницыIndexofPublishResosandMCs1989 2018Joseph Santos GacayanОценок пока нет
- 4-Job Application Form For The Post of LHVДокумент2 страницы4-Job Application Form For The Post of LHVHajveri Photo State SambrialОценок пока нет
- Executive Order No. 385, 1996Документ3 страницыExecutive Order No. 385, 1996VERA FilesОценок пока нет
- Coca-Cola USA PESTLE Analysis (Presentation)Документ8 страницCoca-Cola USA PESTLE Analysis (Presentation)anabia19Оценок пока нет
- Ontario Sunshine List: Other - 2013Документ105 страницOntario Sunshine List: Other - 2013Gillian Grace100% (1)
- Travels Through The Empire oДокумент63 страницыTravels Through The Empire osimonОценок пока нет
- State of Barangay Governance Report (SBGR) CY 2018: Barangay Carpintero Tumauini IsabelaДокумент59 страницState of Barangay Governance Report (SBGR) CY 2018: Barangay Carpintero Tumauini IsabelaJoel SacdalОценок пока нет
- Workout ChartДокумент4 страницыWorkout Chartapi-330453528Оценок пока нет
- Module 5 Identifying HazardsДокумент4 страницыModule 5 Identifying HazardstucaharaОценок пока нет
- Blue Shield CA Employee Enrollment Template v20160101Документ8 страницBlue Shield CA Employee Enrollment Template v20160101Anonymous RLktVcОценок пока нет
- Em American Journal of Infection Control em ObjДокумент2 страницыEm American Journal of Infection Control em ObjKhadiga AhmadОценок пока нет
- Risk Register AllLevelsДокумент5 страницRisk Register AllLevelsSam Atia100% (1)
- Press Conference Addressed by Patriotic Forum For Accountable GovernanceДокумент6 страницPress Conference Addressed by Patriotic Forum For Accountable GovernanceGertrude OtchereОценок пока нет
- Defending Environmental Rights in the Face of RollbacksДокумент20 страницDefending Environmental Rights in the Face of RollbacksAliyan RazzaqОценок пока нет
- Iran IssuesДокумент3 страницыIran IssuesMichelle ChedaОценок пока нет