Вам также может понравиться
- Hip and Knee ArthritisДокумент7 страницHip and Knee ArthritisIndah MirasariОценок пока нет
- Medicine The American Journal of SportsДокумент7 страницMedicine The American Journal of SportsJohann Sebastian CruzОценок пока нет
- 16 HedtДокумент9 страниц16 HedtFederico BristotОценок пока нет
- Y-Balance Test: A Reliability Study Involving Multiple RatersДокумент7 страницY-Balance Test: A Reliability Study Involving Multiple RatersInaauliahanОценок пока нет
- MRI, Força de ExtensoresДокумент16 страницMRI, Força de ExtensoresRosaneLacerdaОценок пока нет
- 2016 Baseline Time To StabilizationДокумент5 страниц2016 Baseline Time To Stabilizationktan.lboroОценок пока нет
- Stromback 2018Документ10 страницStromback 2018Nicolás Ayelef ParraguezОценок пока нет
- Footstrike Angle Cut-Off Values To Classify Footstrike Pattern in RunnersДокумент12 страницFootstrike Angle Cut-Off Values To Classify Footstrike Pattern in RunnersAnggia PОценок пока нет
- Bradley J. Warr 2015Документ5 страницBradley J. Warr 2015Abdelghani MILIANIОценок пока нет
- Sports Injuries of the Foot: Evolving Diagnosis and TreatmentОт EverandSports Injuries of the Foot: Evolving Diagnosis and TreatmentОценок пока нет
- Overview of Running Injuries of The Lower ExtremityДокумент47 страницOverview of Running Injuries of The Lower ExtremityGuardito PequeñoОценок пока нет
- Historial de Lesiones, Sexo y Rendimiento FMS y La Prueba de Equilibrio YДокумент11 страницHistorial de Lesiones, Sexo y Rendimiento FMS y La Prueba de Equilibrio Ycontact.movementsiteОценок пока нет
- Abductor Strenght in Relation With Sports InjuriesДокумент7 страницAbductor Strenght in Relation With Sports InjuriespetrОценок пока нет
- Ijspt 14 192Документ12 страницIjspt 14 192adi pranotoОценок пока нет
- Bushman 2015Документ9 страницBushman 2015Alex SuarezОценок пока нет
- 2012 Daoud Injuries and Foot S 1Документ39 страниц2012 Daoud Injuries and Foot S 1BillVLeeОценок пока нет
- (2017) Running Does Not Increase Symptoms or Structural Progression in People With Knee Osteoarthritis - Data From The Osteoarthritis InitiativeДокумент8 страниц(2017) Running Does Not Increase Symptoms or Structural Progression in People With Knee Osteoarthritis - Data From The Osteoarthritis Initiativecalixto1995Оценок пока нет
- Are Aberrant Running Biomechanics A Risk Factor For Hamstring Strain Injury? A Systematic ReviewДокумент1 страницаAre Aberrant Running Biomechanics A Risk Factor For Hamstring Strain Injury? A Systematic ReviewDisОценок пока нет
- 1 s2.0 S1466853X24000257Документ6 страниц1 s2.0 S1466853X24000257Verónica Obando ToroОценок пока нет
- Osteoporosis Draft Evidence ReviewДокумент397 страницOsteoporosis Draft Evidence ReviewChon ChiОценок пока нет
- Riesgos de HalterofiliaДокумент10 страницRiesgos de HalterofiliaSamuel InfanteОценок пока нет
- Return To Running BolthouseДокумент9 страницReturn To Running BolthouseAriana IorgaОценок пока нет
- Approach Sports Health: A MultidisciplinaryДокумент8 страницApproach Sports Health: A MultidisciplinaryLorena WinklerОценок пока нет
- Shoulder InjuriesДокумент8 страницShoulder InjurieswernsickleОценок пока нет
- Medicine The American Journal of Sports: Diagnosis of Acute Groin Injuries: A Prospective Study of 110 AthletesДокумент9 страницMedicine The American Journal of Sports: Diagnosis of Acute Groin Injuries: A Prospective Study of 110 AthletesomingОценок пока нет
- 2011 - Prevalence of Nonfunctional Overreaching Overtraining in Young English Athletes - Matos Et Al - MedSciSportsExercДокумент9 страниц2011 - Prevalence of Nonfunctional Overreaching Overtraining in Young English Athletes - Matos Et Al - MedSciSportsExercBilingual Physical Education ClassesОценок пока нет
- Resistance Ex Bone TurnoverДокумент7 страницResistance Ex Bone TurnoverHari25885Оценок пока нет
- Canadian Academy of Sport and Exercise Medicine.11Документ5 страницCanadian Academy of Sport and Exercise Medicine.11Diego PonceОценок пока нет
- Prevalence of Back Pain in Sports A Systematic Review of The LiteratureДокумент25 страницPrevalence of Back Pain in Sports A Systematic Review of The LiteratureSamuelОценок пока нет
- Boosting in Athletes With High-Level Spi PDFДокумент20 страницBoosting in Athletes With High-Level Spi PDFKaterina HatzОценок пока нет
- Tennis Elbow JOSPT ArticleДокумент11 страницTennis Elbow JOSPT ArticleHasan RahmanОценок пока нет
- Kinesiology The Mechanics and Pathomechanics of Human Movement 3rd Edition Ebook PDFДокумент62 страницыKinesiology The Mechanics and Pathomechanics of Human Movement 3rd Edition Ebook PDFbruce.glinski869100% (47)
- Bone Stress Injury Middle Age RunnersДокумент28 страницBone Stress Injury Middle Age RunnersAnggia PОценок пока нет
- Incremental Increases in Non Exercise Estimated Fitness Reduce Subsequent Depressive SymptomsДокумент9 страницIncremental Increases in Non Exercise Estimated Fitness Reduce Subsequent Depressive SymptomsAthenaeum Scientific PublishersОценок пока нет
- (2023) Effects of Running On The Development of Knee OsteoarthritisДокумент6 страниц(2023) Effects of Running On The Development of Knee Osteoarthritiscalixto1995Оценок пока нет
- The Female Athlete Triad: A Clinical GuideОт EverandThe Female Athlete Triad: A Clinical GuideCatherine M. GordonОценок пока нет
- Gymnastics Medicine: Evaluation, Management and RehabilitationОт EverandGymnastics Medicine: Evaluation, Management and RehabilitationОценок пока нет
- Fundamental Movement and DynamicДокумент9 страницFundamental Movement and DynamicYoh ChenОценок пока нет
- 1 s2.0 S2666506920300225 MainДокумент7 страниц1 s2.0 S2666506920300225 MainDela AgustinaОценок пока нет
- SLAP Tear Management in AthletesДокумент11 страницSLAP Tear Management in AthletesErnesto Dávila RamírezОценок пока нет
- Reduced Incidence of Cardiac Arrhythmias in Walkers and RunnersДокумент7 страницReduced Incidence of Cardiac Arrhythmias in Walkers and RunnersJHOAN ANDRÉS PALACIOS VALDESОценок пока нет
- An Emerging Pattern of Subtrochanteric Stress FracturesДокумент6 страницAn Emerging Pattern of Subtrochanteric Stress FracturesAlejandro OrduzОценок пока нет
- Short Bicep Femoris Fascicles and Ecc Knee Flexor Weakness Increase Hamstring Injury - Soccer Cohort StueyДокумент13 страницShort Bicep Femoris Fascicles and Ecc Knee Flexor Weakness Increase Hamstring Injury - Soccer Cohort StueywernsickleОценок пока нет
- Ferraz Et Al. 2017 PDFДокумент36 страницFerraz Et Al. 2017 PDFmatheus ramosОценок пока нет
- 'Shin Splints' - Medial Tibial Stress Syndrome: A Review of The LiteratureДокумент15 страниц'Shin Splints' - Medial Tibial Stress Syndrome: A Review of The LiteratureAryani WardaniОценок пока нет
- Blood Ow Restriction Augments The Skeletal Muscle Response During Very Low-Load Resistance Exercise To Volitional FailureДокумент14 страницBlood Ow Restriction Augments The Skeletal Muscle Response During Very Low-Load Resistance Exercise To Volitional FailureFabiano LacerdaОценок пока нет
- Fresults From The Health, Aging and BodyДокумент6 страницFresults From The Health, Aging and BodyNikolas EdwinОценок пока нет
- 370 FullДокумент5 страниц370 Fulln gautamОценок пока нет
- J Jstrokecerebrovasdis 2016 10 018Документ8 страницJ Jstrokecerebrovasdis 2016 10 018gilangОценок пока нет
- Annual Compilation of Wrestling ResearchДокумент56 страницAnnual Compilation of Wrestling ResearchSergio OliveiraОценок пока нет
- Impact-Related Ground Reaction Forces Are More Strongly Associated With Some Running Injuries Than OthersДокумент9 страницImpact-Related Ground Reaction Forces Are More Strongly Associated With Some Running Injuries Than OthersAriene RibeiroОценок пока нет
- Prevention of Medial Tibial Stress SyndromeДокумент7 страницPrevention of Medial Tibial Stress Syndromeapi-367371787Оценок пока нет
- 2017 ATS 6mwtДокумент32 страницы2017 ATS 6mwtOrion JohnОценок пока нет
- Tez Ingilizce Makale - EditedДокумент20 страницTez Ingilizce Makale - EditedStefanny DamacinОценок пока нет
- Isquiotibiales TestДокумент6 страницIsquiotibiales TestHugo TintiОценок пока нет
- JEPonlineOCTOBER 5 2017 Montes PDFДокумент7 страницJEPonlineOCTOBER 5 2017 Montes PDFAndrés MenesesОценок пока нет
- Rehabilitation and Return To Sport After Hamstring Strain InjuryДокумент9 страницRehabilitation and Return To Sport After Hamstring Strain InjuryJonОценок пока нет
- Anthropometric and Morphological Characteristics of RunnersДокумент6 страницAnthropometric and Morphological Characteristics of RunnersMarcelo NogueraОценок пока нет
- Journal of Yoga & Physical Therapy: Designing A Return To Training Model For Professional Athletes After Sport InjuryДокумент2 страницыJournal of Yoga & Physical Therapy: Designing A Return To Training Model For Professional Athletes After Sport InjuryCarlos Martín De RosasОценок пока нет
- Medial Tibial Stress SyndromeДокумент18 страницMedial Tibial Stress SyndromeCarlos Martín De RosasОценок пока нет
- 10.1177 1941738113481200 PDFДокумент9 страниц10.1177 1941738113481200 PDFCarlos Martín De RosasОценок пока нет
- Periodization of Training For Team Sports Athletes.9Документ11 страницPeriodization of Training For Team Sports Athletes.9Carlos Martín De Rosas100% (1)
- 10 1016@j Jpain 2009 04 017Документ9 страниц10 1016@j Jpain 2009 04 017Carlos Martín De RosasОценок пока нет
- Alimentacion NutricionДокумент41 страницаAlimentacion NutricionCarlos Martín De RosasОценок пока нет
- Time Before Return To Play For The Most Common Injuries in Professional Football: A 16-Year Follow-Up of The UEFA Elite Club Injury StudyДокумент6 страницTime Before Return To Play For The Most Common Injuries in Professional Football: A 16-Year Follow-Up of The UEFA Elite Club Injury StudyCarlos Martín De RosasОценок пока нет
- Meta-Analysis of The Effect of Exercise Interventions On Fitness Outcomes Among Adults With Type 1 and Type 2 DiabetesДокумент10 страницMeta-Analysis of The Effect of Exercise Interventions On Fitness Outcomes Among Adults With Type 1 and Type 2 DiabetesCarlos Martín De RosasОценок пока нет
- The Rotator Interval Pathology and ManagementДокумент12 страницThe Rotator Interval Pathology and ManagementCarlos Martín De RosasОценок пока нет
- Johnson 2007Документ12 страницJohnson 2007Carlos Martín De RosasОценок пока нет
- Clinical Aspects of Physical Exercise For Diabetes/metabolic SyndromeДокумент5 страницClinical Aspects of Physical Exercise For Diabetes/metabolic Syndromeprofesi nersОценок пока нет
- Physical Activity Exercise Training in Type 2Документ5 страницPhysical Activity Exercise Training in Type 2Carlos Martín De Rosas100% (1)
- The Effect of Anterior Versus Posterior Glide Joint MobilizationДокумент6 страницThe Effect of Anterior Versus Posterior Glide Joint MobilizationCarlos Martín De RosasОценок пока нет
- Diagnosis and Management of Adhesive CapsulitisДокумент10 страницDiagnosis and Management of Adhesive CapsulitisCarlos Martín De RosasОценок пока нет
- Carville2007 PDFДокумент7 страницCarville2007 PDFCarlos Martín De RosasОценок пока нет
- Lumbar Instability Ands Exercises 2000Документ11 страницLumbar Instability Ands Exercises 2000Francisco Javier Quinteros GarcíaОценок пока нет
- Supplements 75 6Документ17 страницSupplements 75 6Carlos Martín De RosasОценок пока нет
- Johnson 2007Документ12 страницJohnson 2007Carlos Martín De RosasОценок пока нет
- Gait Parameters Associated With Hallux ValgusДокумент12 страницGait Parameters Associated With Hallux ValgusCarlos Martín De RosasОценок пока нет
- Ankle - Tibial Stress InjuriesДокумент9 страницAnkle - Tibial Stress InjuriesCarlos Martín De RosasОценок пока нет
- Avances LCA WilkДокумент19 страницAvances LCA WilkCarlos Martín De RosasОценок пока нет
- Inestab Anterior HombroДокумент11 страницInestab Anterior HombroCarlos Martín De RosasОценок пока нет
- Medial Tibial Stress SyndromeДокумент18 страницMedial Tibial Stress SyndromeCarlos Martín De RosasОценок пока нет
- BR J Sports Med 2016 Ardern Bjsports 2016 096278Документ13 страницBR J Sports Med 2016 Ardern Bjsports 2016 096278Carlos Martín De RosasОценок пока нет
- CapsДокумент14 страницCapsCarlos Martín De RosasОценок пока нет
- Manipulation of The Cervical Spine A Systematic Review of Case Reports of Serious Adverse Events1995-2001Документ5 страницManipulation of The Cervical Spine A Systematic Review of Case Reports of Serious Adverse Events1995-2001Carlos Martín De RosasОценок пока нет
- Protocol 1 Achilles Tendon Repair v5Документ2 страницыProtocol 1 Achilles Tendon Repair v5Carlos Martín De RosasОценок пока нет
- Resistencia Localizada para Activar Selectivamente El Semiespinal Cervical en Pacientes Con Dolor Cervical 2012Документ5 страницResistencia Localizada para Activar Selectivamente El Semiespinal Cervical en Pacientes Con Dolor Cervical 2012Carlos Martín De RosasОценок пока нет
- Osteotomia TibialДокумент2 страницыOsteotomia TibialCarlos Martín De RosasОценок пока нет
- Kampa VataДокумент27 страницKampa VataAditya Tak100% (1)
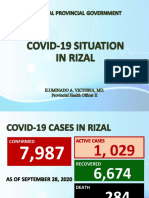
- Covid19 Situation in RizalДокумент23 страницыCovid19 Situation in RizalToni Quitalig GamezОценок пока нет
- Health Services in WAДокумент10 страницHealth Services in WAlaureeateОценок пока нет
- Diagnosis and Management of Subarachnoid HemorrhageДокумент25 страницDiagnosis and Management of Subarachnoid HemorrhageMisael ClintonОценок пока нет
- Pedia Small Notebook Edited PDFДокумент17 страницPedia Small Notebook Edited PDFAshОценок пока нет
- Ebook - Yoga - The Science of BreathДокумент2 страницыEbook - Yoga - The Science of BreathGabriel CiocanОценок пока нет
- Drug Descrubrimiento de FarmacosДокумент302 страницыDrug Descrubrimiento de FarmacosdavidОценок пока нет
- 2016 S 0042 108641 PDFДокумент29 страниц2016 S 0042 108641 PDFMadalina StoicescuОценок пока нет
- Lactated Ringer'sДокумент7 страницLactated Ringer'sPPLaloОценок пока нет
- 2023 Aaha Senior Care Guidelines For Dogs and CatsДокумент21 страница2023 Aaha Senior Care Guidelines For Dogs and CatsisvpОценок пока нет
- Sodium Chloride (Rock Salt) MSDS: Section 1: Chemical Product and Company IdentificationДокумент6 страницSodium Chloride (Rock Salt) MSDS: Section 1: Chemical Product and Company IdentificationMohamed MaghawryОценок пока нет
- Basic Principles of Normal ECG: Prepared By: Ben Ryan Jucay SauceДокумент25 страницBasic Principles of Normal ECG: Prepared By: Ben Ryan Jucay SauceSoySauceОценок пока нет
- Post-Operative Abdominal Infections: Epidemiology, Operational Definitions, and OutcomesДокумент10 страницPost-Operative Abdominal Infections: Epidemiology, Operational Definitions, and OutcomesJared CossioОценок пока нет
- D. Santhi Krupa, Et Al IJAPRДокумент6 страницD. Santhi Krupa, Et Al IJAPRAtraoОценок пока нет
- Spring Meadows Hospital VsДокумент10 страницSpring Meadows Hospital VsManoj Kumar MОценок пока нет
- OB Gyne HistoryДокумент2 страницыOB Gyne HistoryNeil Victor Ongco PajugotОценок пока нет
- Ais YesДокумент15 страницAis YesLauriz Dillumas MachonОценок пока нет
- Mic Eales A Visual Enquiry Into SuicideДокумент4 страницыMic Eales A Visual Enquiry Into Suicidemaribolla8015Оценок пока нет
- No Kode SAP Lokasi Rak Nama ProdukДокумент117 страницNo Kode SAP Lokasi Rak Nama ProdukKimia ByPass TabananОценок пока нет
- 04-09-12 EditionДокумент28 страниц04-09-12 EditionSan Mateo Daily JournalОценок пока нет
- Johnson & Johnson Tylenol CrisisДокумент21 страницаJohnson & Johnson Tylenol CrisisArnab Chatterjee100% (2)
- Windy WigaДокумент2 страницыWindy WigaWindy wigaОценок пока нет
- Rectal ProlapseДокумент9 страницRectal ProlapseAnjani Putri RetnaninggalihОценок пока нет
- Skin Care Plan: Nu Derm Protocol ForДокумент7 страницSkin Care Plan: Nu Derm Protocol ForsheilaОценок пока нет
- HerbalismДокумент18 страницHerbalismmieОценок пока нет
- LidocaineДокумент11 страницLidocaineStanford AnesthesiaОценок пока нет
- Binge EatingДокумент18 страницBinge EatingIuliana IgnatОценок пока нет
- Theraputic UltrasoundДокумент64 страницыTheraputic UltrasoundRoshni KhanОценок пока нет
- Negative Effects of Video GamesДокумент5 страницNegative Effects of Video GamesMadeОценок пока нет