Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- DynsimДокумент22 страницыDynsimAbdomatarОценок пока нет
- Specification For Pressure Vessel Plates, Alloy Steel, Manganese-Molybdenum and Manganese-Molybdenum-NickelДокумент4 страницыSpecification For Pressure Vessel Plates, Alloy Steel, Manganese-Molybdenum and Manganese-Molybdenum-NickelmalsttarОценок пока нет
- Geo Sintetik by Dirgatz IndonesiaДокумент6 страницGeo Sintetik by Dirgatz IndonesiabudivinolaОценок пока нет
- Complete Inorganic MarathonДокумент407 страницComplete Inorganic MarathonAdithya kumar JhaОценок пока нет
- Diffusion and Osmosis LabДокумент2 страницыDiffusion and Osmosis LabJustin NgОценок пока нет
- Mass Spectra and IRДокумент7 страницMass Spectra and IRSyed FahimОценок пока нет
- Conductimetric Analysis of Water Soluble Ionic Contamination of Blasting AbrasivesДокумент3 страницыConductimetric Analysis of Water Soluble Ionic Contamination of Blasting AbrasivesCristhian CoariteОценок пока нет
- ProblemsДокумент2 страницыProblemsJoisy Sarco CondoriОценок пока нет
- Banana Stem JuiceДокумент8 страницBanana Stem Juiceईन्द्रनील रायОценок пока нет
- All About Concrete Pavement Joint Design and Construction FINAL 100214Документ141 страницаAll About Concrete Pavement Joint Design and Construction FINAL 100214tbanano100% (2)
- THE HIGH PRESSURE ROLLER PRESSДокумент27 страницTHE HIGH PRESSURE ROLLER PRESSThaigroup Cement100% (10)
- 计量泵metering pump PDFДокумент43 страницы计量泵metering pump PDFAnonymous Tj3ApePIrОценок пока нет
- Asme InterpretationДокумент72 страницыAsme Interpretationbbmoksh100% (2)
- DAO 2016-08 Features and CAPДокумент64 страницыDAO 2016-08 Features and CAPDianne Kristine Avila100% (4)
- Material QuizДокумент22 страницыMaterial QuizMr Nerd100% (3)
- Corrosion Protection Properties and Interfacial Adhesion MechanismДокумент20 страницCorrosion Protection Properties and Interfacial Adhesion MechanismMaría Flores ToledoОценок пока нет
- Distillation Column Tray Selection & Sizing - 1 - Separation TechnologiesДокумент18 страницDistillation Column Tray Selection & Sizing - 1 - Separation TechnologiesOmesh Borole100% (1)
- Rules and Refulation For The Classification of Special Service Craft July 2015 - Piping Systems and Presure Plant - ConstructionДокумент4 страницыRules and Refulation For The Classification of Special Service Craft July 2015 - Piping Systems and Presure Plant - ConstructionmarboledtОценок пока нет
- b28113433 PDFДокумент202 страницыb28113433 PDFJuthika GogoiОценок пока нет
- Enthalpy Method PDFДокумент2 страницыEnthalpy Method PDFsimmaОценок пока нет
- Chemigrams and CyanotypesДокумент4 страницыChemigrams and Cyanotypesapi-481057728Оценок пока нет
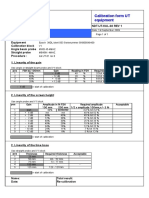
- Calibration Sheet Ultrasonic Test EquipmentДокумент1 страницаCalibration Sheet Ultrasonic Test EquipmentjohnОценок пока нет
- What Is The Major Function of The Coating On An Arc Welding ElectrodeДокумент7 страницWhat Is The Major Function of The Coating On An Arc Welding ElectrodeElham Jaraine Garcia Lpt100% (4)
- Gemstone and Crystal Reference Book EnglishДокумент29 страницGemstone and Crystal Reference Book Englishsandu_livia100% (1)
- Drugs of Hindustan PDFДокумент382 страницыDrugs of Hindustan PDFdr madan mohan gundu100% (1)
- Bracing Requirements For Elastic Steel BeamsДокумент87 страницBracing Requirements For Elastic Steel BeamsbiomechanicsОценок пока нет
- Mid Term Presentation - Anish Kumar DakshДокумент23 страницыMid Term Presentation - Anish Kumar DakshShubhadeep MajumdarОценок пока нет
- Validation of Raw MaterialДокумент22 страницыValidation of Raw MaterialPrima RamadhaniОценок пока нет
- Determining Cation Exchange Capacity: A New Procedure For Calcareous and Gypsiferous SoilsДокумент5 страницDetermining Cation Exchange Capacity: A New Procedure For Calcareous and Gypsiferous SoilsM. Yusuf HermawanОценок пока нет
- Chemistry Assessment - Task 2 Report (Update 3)Документ15 страницChemistry Assessment - Task 2 Report (Update 3)kaylasadgrove4Оценок пока нет