Вам также может понравиться
- Uw2 Ome: Online Meded Su2M: Mim BB HimДокумент1 страницаUw2 Ome: Online Meded Su2M: Mim BB HimvinОценок пока нет
- High Yield Internal Medicine Compatible VersionДокумент100 страницHigh Yield Internal Medicine Compatible VersionAhsan X Baig100% (5)
- AnatomyДокумент4 страницыAnatomyvinОценок пока нет
- TirukuralДокумент623 страницыTirukuralvin100% (2)
- High Yield Surgery Compatible Version PDFДокумент77 страницHigh Yield Surgery Compatible Version PDFDuke71% (7)
- Surgical Notes A Pocket Survival GuideДокумент197 страницSurgical Notes A Pocket Survival Guidevin100% (12)
- Feature Hepatitis A Hepatitis B Hepatitis C: Common Name Virus Structure Transmission Onset Incubation Period (Days)Документ2 страницыFeature Hepatitis A Hepatitis B Hepatitis C: Common Name Virus Structure Transmission Onset Incubation Period (Days)vinОценок пока нет
- OMT ReviewДокумент114 страницOMT Reviewvin100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Biology: University of Cambridge International Examinations General Certificate of Education Advanced LevelДокумент36 страницBiology: University of Cambridge International Examinations General Certificate of Education Advanced Levellfwjfw;fwjf;fjОценок пока нет
- AED (Automated External Defibrilation)Документ17 страницAED (Automated External Defibrilation)Ari AsriniОценок пока нет
- Drug Study NubainДокумент2 страницыDrug Study NubainampalОценок пока нет
- Summer Training For Speed: Alwyn Cosgrove's Training Design ProgramДокумент6 страницSummer Training For Speed: Alwyn Cosgrove's Training Design ProgramSteve HeywoodОценок пока нет
- Skin - Structure and Function Flashcards - QuizletДокумент5 страницSkin - Structure and Function Flashcards - QuizletDani AnyikaОценок пока нет
- Worksheet 2 - Hematology - 2020 (11th Ed)Документ3 страницыWorksheet 2 - Hematology - 2020 (11th Ed)ahmadmahdi18mОценок пока нет
- 11 Biology Notes ch05 Morphology of Flowering Plants PDFДокумент7 страниц11 Biology Notes ch05 Morphology of Flowering Plants PDFMeenakshi VenkataramanОценок пока нет
- 12 Biology Notes Ch06 Molecular Basis of InheritanceДокумент6 страниц12 Biology Notes Ch06 Molecular Basis of InheritanceInderpal SinghОценок пока нет
- SalbutamolДокумент5 страницSalbutamolFildehl Janice Bomediano CatipayОценок пока нет
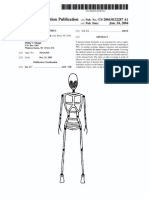
- Patente Endoesqueleto para Sex Doll SiliconaДокумент12 страницPatente Endoesqueleto para Sex Doll SiliconaGabriel De Jesus100% (1)
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALДокумент5 страницPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralОценок пока нет
- Cardiology & Ekgs: Archer Nclex ReviewДокумент59 страницCardiology & Ekgs: Archer Nclex Reviewdaphne farleyОценок пока нет
- Lecture Notes On Biophysics and Bioimaging 2009Документ128 страницLecture Notes On Biophysics and Bioimaging 2009Anonymous 9rJe2lOskx100% (2)
- Integumentary System - NUR1019 - 20sept2022Документ33 страницыIntegumentary System - NUR1019 - 20sept2022琪琪Оценок пока нет
- Patho OTДокумент23 страницыPatho OTBea Y. Bas-ongОценок пока нет
- STSurg NumntДокумент11 страницSTSurg NumntrohiОценок пока нет
- Endocrine Glands RevisedДокумент47 страницEndocrine Glands RevisedXyress Archer GosinganОценок пока нет
- Manor Supplementary Notes PCOGДокумент32 страницыManor Supplementary Notes PCOGBenjamin TОценок пока нет
- Introduction To Health Care 4th Edition Mitchell Solutions Manual DownloadДокумент5 страницIntroduction To Health Care 4th Edition Mitchell Solutions Manual DownloadMark Prindle100% (20)
- CH 03Документ36 страницCH 03abdurОценок пока нет
- PathoДокумент54 страницыPathojohnОценок пока нет
- Uropati ObstruktifДокумент22 страницыUropati ObstruktifEvan Permana100% (1)
- Fisioterapi JurnalДокумент7 страницFisioterapi JurnalAchenk BarcelonistaОценок пока нет
- Early Complications of MIДокумент11 страницEarly Complications of MIjen262004Оценок пока нет
- 11 Ch1208 5127 PDFДокумент25 страниц11 Ch1208 5127 PDFThamarai ElanthirayanОценок пока нет
- Newport, D.J. and Nemeroff, C.B. Neurobiology of Posttraumatic Stress Disorder. Cognitive Neuroscience JAARTALДокумент8 страницNewport, D.J. and Nemeroff, C.B. Neurobiology of Posttraumatic Stress Disorder. Cognitive Neuroscience JAARTALg10564433Оценок пока нет
- Xi - Bio Zoo Question PaperДокумент9 страницXi - Bio Zoo Question PaperVeeramaniОценок пока нет
- NUTRITIONAL MANAGEMENT OF OBESITY & TYPE 2 DIABETES EspenДокумент34 страницыNUTRITIONAL MANAGEMENT OF OBESITY & TYPE 2 DIABETES EspenMarcelo Murillo0% (1)
- Effective Suction-Imporession For Retentive Mand Dentture PDFДокумент24 страницыEffective Suction-Imporession For Retentive Mand Dentture PDFFaheemuddin MuhammadОценок пока нет
- Arterial Tourniquets Anaesthesia Tutorial of The Week 200 11 OCTOBER 2010Документ7 страницArterial Tourniquets Anaesthesia Tutorial of The Week 200 11 OCTOBER 2010tessalaiОценок пока нет