Вам также может понравиться
- SBC Code 303Документ97 страницSBC Code 303dyx90% (10)
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderОт EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderОценок пока нет
- Proteinuria BasicMechanismsPathophys PDFДокумент147 страницProteinuria BasicMechanismsPathophys PDFLedira Dara IsmiОценок пока нет
- Complementary and Alternative Medical Lab Testing Part 8: UrologyОт EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyРейтинг: 3 из 5 звезд3/5 (1)
- Tom Bisio - Ba Gua Nei Gong Marrow Washing Nei GongДокумент111 страницTom Bisio - Ba Gua Nei Gong Marrow Washing Nei GongIsidro Castaño Marquez75% (4)
- Soil Guidance NotesДокумент18 страницSoil Guidance Notesసాయిమహేష్రెడ్డిఆవులОценок пока нет
- An International Railway Project - A Project Management Case StudyДокумент9 страницAn International Railway Project - A Project Management Case StudySourav NathОценок пока нет
- 2 Tietz 2012 Kidney Function TestsДокумент39 страниц2 Tietz 2012 Kidney Function TestsIvana BajunovicОценок пока нет
- Integration Procedure of Telecom System WHP andДокумент53 страницыIntegration Procedure of Telecom System WHP andselamet riantoОценок пока нет
- Rural Poultry Management GuideДокумент7 страницRural Poultry Management Guideసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Clinical Approach To Advanced Renal Function Tes Ting in Dogs and CA TsДокумент16 страницClinical Approach To Advanced Renal Function Tes Ting in Dogs and CA Tsl.fernandagonzalez97Оценок пока нет
- Traditional Renal Biomarkers and New Approaches To DiagnosticsДокумент3 страницыTraditional Renal Biomarkers and New Approaches To DiagnosticsAlessandra SantanaОценок пока нет
- Abordaje de PX Con Enf RenalДокумент12 страницAbordaje de PX Con Enf Renalcleooatra mairenaОценок пока нет
- Integral University, Lucknow: Session:2019-2020Документ6 страницIntegral University, Lucknow: Session:2019-2020Kausal VermaОценок пока нет
- Primary Care Approach To Proteinuria: Amir Said Alizadeh Naderi, MD, and Robert F. Reilly, MDДокумент6 страницPrimary Care Approach To Proteinuria: Amir Said Alizadeh Naderi, MD, and Robert F. Reilly, MDraviibtОценок пока нет
- The Relation Between Liver Histopathology and GGT Levels in Viral Hepatitis: More Important in Hepatitis BДокумент5 страницThe Relation Between Liver Histopathology and GGT Levels in Viral Hepatitis: More Important in Hepatitis BTanveerОценок пока нет
- Salivary FRAP As A Marker of Chronic Kidney Disease Progression in ChildrenДокумент18 страницSalivary FRAP As A Marker of Chronic Kidney Disease Progression in ChildrenfghdhmdkhОценок пока нет
- Urinary Biomarkers For Acute Kidney Injury in DogsДокумент13 страницUrinary Biomarkers For Acute Kidney Injury in Dogsheidy acostaОценок пока нет
- Study of Serum Gamma Glutamyl Transferase As A Diagnostic Marker in Alcoholic HepatitisДокумент3 страницыStudy of Serum Gamma Glutamyl Transferase As A Diagnostic Marker in Alcoholic HepatitisIOSR Journal of PharmacyОценок пока нет
- Acta Veterinaria ScandinavicaДокумент6 страницActa Veterinaria ScandinavicaMarilú ValdepeñaОценок пока нет
- The New Age of Renal Biomarkers - Does SDMA Solve All of Our ProblemsДокумент11 страницThe New Age of Renal Biomarkers - Does SDMA Solve All of Our ProblemsCabinet VeterinarОценок пока нет
- Spider Angiomas in Patients With Liver Cirrhosis: Role of Vascular Endothelial Growth Factor and Basic Fibroblast Growth FactorДокумент4 страницыSpider Angiomas in Patients With Liver Cirrhosis: Role of Vascular Endothelial Growth Factor and Basic Fibroblast Growth FactorChrizzna HaryantoОценок пока нет
- Apendice Falla Renal. y AlbuminuriaДокумент20 страницApendice Falla Renal. y AlbuminuriajoelОценок пока нет
- Early Urinary Markers Predict Kidney Disease in DiabetesДокумент11 страницEarly Urinary Markers Predict Kidney Disease in DiabetesFelipe SangiovanniОценок пока нет
- Interpretation of The eGFR Jul 07Документ8 страницInterpretation of The eGFR Jul 07Danielcc LeeОценок пока нет
- Vitamin D, PTH, Calcium, and Phosphorus Abnormalities in CKD PatientsДокумент8 страницVitamin D, PTH, Calcium, and Phosphorus Abnormalities in CKD PatientsCristian CozmaОценок пока нет
- A Case Study On Urinalysis and Body FluidsДокумент17 страницA Case Study On Urinalysis and Body Fluidsrakish16Оценок пока нет
- 10 1111@eve 13373Документ10 страниц10 1111@eve 13373ccamachoОценок пока нет
- The Role of Biomarkers inДокумент16 страницThe Role of Biomarkers inSoniamartilovaОценок пока нет
- Primary Care Approach To ProteinuriaДокумент6 страницPrimary Care Approach To Proteinuriadanny17phОценок пока нет
- Kidneydiseaseandthe Nexusofchronickidney DiseaseandacutekidneyinjuryДокумент33 страницыKidneydiseaseandthe Nexusofchronickidney DiseaseandacutekidneyinjuryMardauc AnaidОценок пока нет
- Jvim 29 028Документ7 страницJvim 29 028Marilyn Patricia Abello GarciaОценок пока нет
- Pancreatitis in Dogs and Cats - Digestive System - Merck Veterinary ManualДокумент6 страницPancreatitis in Dogs and Cats - Digestive System - Merck Veterinary Manualchihsiang chenОценок пока нет
- Proteinuria in Dogs and CatsДокумент9 страницProteinuria in Dogs and Catsfreak009Оценок пока нет
- ACPN AbstractsДокумент21 страницаACPN AbstractsPediatric NephrologyОценок пока нет
- Awad 2003Документ5 страницAwad 2003Jansen ChОценок пока нет
- Renal PhysiologyДокумент7 страницRenal PhysiologyLucas TheotonioОценок пока нет
- Plasma Leptin Levels in Rats With PancreatitisДокумент6 страницPlasma Leptin Levels in Rats With PancreatitisAndykaYayanSetiawanОценок пока нет
- Proteinuria in Adults - A Diagnostic Approach - AAFPДокумент12 страницProteinuria in Adults - A Diagnostic Approach - AAFPXeric CedoОценок пока нет
- Paper 1Документ16 страницPaper 1constanzanazarethОценок пока нет
- Hepatic Computed Tomography and Cholangiography by Use of Gadoxetic Acid in Healthy CatsДокумент11 страницHepatic Computed Tomography and Cholangiography by Use of Gadoxetic Acid in Healthy CatsAlejandro Estrada RiosОценок пока нет
- Corea Del Sur 2019 SODIUMGLUCOSE COTRANSPORTER 2 INHIBOTOR FORДокумент1 страницаCorea Del Sur 2019 SODIUMGLUCOSE COTRANSPORTER 2 INHIBOTOR FORLaura GarciaОценок пока нет
- Hyperuricemia Is Associated With Hypertension, Obesity, and Albuminuria in Children With Chronic Kidney DiseaseДокумент5 страницHyperuricemia Is Associated With Hypertension, Obesity, and Albuminuria in Children With Chronic Kidney DiseaseMuh Husni RifaiОценок пока нет
- 1 s2.0 S2468024919300890 MainДокумент9 страниц1 s2.0 S2468024919300890 MainGabriela PachecoОценок пока нет
- Gene Therapy For Type 1 Diabetes Mellitus in Rats by Gastrointestinal Administration of Chitosan Nanoparticles Containing Human Insulin GeneДокумент7 страницGene Therapy For Type 1 Diabetes Mellitus in Rats by Gastrointestinal Administration of Chitosan Nanoparticles Containing Human Insulin GenesaifudinОценок пока нет
- Evaluation of Coagulation Parameters in Dogs With Gallbladder Mucoceles - Veterinary Internal Medicne - 2021 - PavlickДокумент10 страницEvaluation of Coagulation Parameters in Dogs With Gallbladder Mucoceles - Veterinary Internal Medicne - 2021 - PavlickEduardo SantamaríaОценок пока нет
- Jurnal Thalassemia 4Документ10 страницJurnal Thalassemia 4Lina AnisaОценок пока нет
- A Case of Aspartate Aminotransferase MacroenzymeДокумент3 страницыA Case of Aspartate Aminotransferase MacroenzymeOlfiany Laurenzia PongohОценок пока нет
- Oral Calcitriol For Reduction of Proteinuria in Patients With Iga Nephropathy: A Randomized Controlled TrialДокумент8 страницOral Calcitriol For Reduction of Proteinuria in Patients With Iga Nephropathy: A Randomized Controlled Trialjustin_saneОценок пока нет
- Diagnostic Utility of Protein To Creatinine RatioДокумент21 страницаDiagnostic Utility of Protein To Creatinine RatioDinda YenviartiОценок пока нет
- Screening Tool For Proteinuria in Lupus NephritisДокумент7 страницScreening Tool For Proteinuria in Lupus NephritisM Dwi SuprayogiОценок пока нет
- (03241750 - Acta Medica Bulgarica) The Heparanase Inhibitor (Sulodexide) Decreases Urine Glycosaminoglycan Excretion and Mitigates Functional and Histological Renal Damages in Diabetic RatsДокумент6 страниц(03241750 - Acta Medica Bulgarica) The Heparanase Inhibitor (Sulodexide) Decreases Urine Glycosaminoglycan Excretion and Mitigates Functional and Histological Renal Damages in Diabetic RatsTeodorОценок пока нет
- World Journal Of: HepatologyДокумент12 страницWorld Journal Of: HepatologywiwiОценок пока нет
- Prediction model identifies chronic kidney disease risk factorsДокумент14 страницPrediction model identifies chronic kidney disease risk factorsjuantoОценок пока нет
- A Laboratory Diagnostic Approach To Hepatobiliary Disease in Small AnimalsДокумент17 страницA Laboratory Diagnostic Approach To Hepatobiliary Disease in Small Animalsl.fernandagonzalez97Оценок пока нет
- Journal Presentation: The New England Journal of Medicine Case Records of The Massachusetts General HospitalДокумент49 страницJournal Presentation: The New England Journal of Medicine Case Records of The Massachusetts General HospitalSomnath SenguptaОценок пока нет
- Pioglitazone Reduces Cisplatin Nephrotoxicity and Boosts Anticancer ActivityДокумент33 страницыPioglitazone Reduces Cisplatin Nephrotoxicity and Boosts Anticancer ActivityIan GabritoОценок пока нет
- Novel Biomarkers of Renal FunctionДокумент4 страницыNovel Biomarkers of Renal Functionramesh3135kumar100% (1)
- Association of Serum Uric AcidДокумент40 страницAssociation of Serum Uric AcidWoro Hapsari WahyuningrumОценок пока нет
- RCT ArticleДокумент8 страницRCT ArticleelpisОценок пока нет
- Materials and MethodsДокумент3 страницыMaterials and MethodssurtitejoОценок пока нет
- Proteinuria Pada Anak AnakДокумент7 страницProteinuria Pada Anak Anaklathifa nabilaОценок пока нет
- Case Report Glycogenic Hepatopathy in Type 1 Diabetes MellitusДокумент4 страницыCase Report Glycogenic Hepatopathy in Type 1 Diabetes MellitusCarlos Alberto Rodriguez ValbuenaОценок пока нет
- Presymptomatic Hyperuricemia Risks and TreatmentДокумент46 страницPresymptomatic Hyperuricemia Risks and TreatmentDivya Shree100% (1)
- Veterinary Clinical Pathol - 2018 - Hokamp - Correlation of Electrophoretic Urine Protein Banding Patterns With Severity ofДокумент10 страницVeterinary Clinical Pathol - 2018 - Hokamp - Correlation of Electrophoretic Urine Protein Banding Patterns With Severity ofLeandroОценок пока нет
- Diagnostic Pathology of Hematopoietic Disorders of Spleen and LiverОт EverandDiagnostic Pathology of Hematopoietic Disorders of Spleen and LiverОценок пока нет
- RRWheat PoultryscienceДокумент10 страницRRWheat Poultryscienceసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Importance of Carrier For Feed Premixes ProductionДокумент5 страницImportance of Carrier For Feed Premixes Productionసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Key Considerations For Appraisal of DPR and Checklist of DPR ComponentsДокумент6 страницKey Considerations For Appraisal of DPR and Checklist of DPR Componentsసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Animal Husbandary Assistant PDFДокумент39 страницAnimal Husbandary Assistant PDFSRINIVASARAO BELLAMKONDAОценок пока нет
- Chicken Respiratory AnatomyДокумент4 страницыChicken Respiratory Anatomyసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Avian Respiratory System - EXtensionДокумент3 страницыAvian Respiratory System - EXtensionసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Ipuru Mandal GPS ListДокумент1 страницаIpuru Mandal GPS Listసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Avian Respiratory System - EXtensionДокумент3 страницыAvian Respiratory System - EXtensionసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Ipuru Mandal GPS ListДокумент1 страницаIpuru Mandal GPS Listసాయిమహేష్రెడ్డిఆవులОценок пока нет
- ASPIRE Guidelines FinalДокумент48 страницASPIRE Guidelines FinalMd RaihanОценок пока нет
- Avian Respiratory System: Jacquie Jacob and Tony Pescatore, Animal SciencesДокумент2 страницыAvian Respiratory System: Jacquie Jacob and Tony Pescatore, Animal Sciencesసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Avian Respiratory System - EXtensionДокумент3 страницыAvian Respiratory System - EXtensionసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Houston-2011-The Journal of Clinical HypertensionДокумент7 страницHouston-2011-The Journal of Clinical Hypertensionసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Career Opportunities in AgricultureДокумент3 страницыCareer Opportunities in Agricultureసాయిమహేష్రెడ్డిఆవులОценок пока нет
- User'S Manual FOR Candidates FOR: Online Registration & Choice FillingДокумент16 страницUser'S Manual FOR Candidates FOR: Online Registration & Choice Fillingసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Flavonoid: 1 BiosynthesisДокумент12 страницFlavonoid: 1 Biosynthesisసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Kidney Biopsy, Histo, UpcДокумент9 страницKidney Biopsy, Histo, Upcసాయిమహేష్రెడ్డిఆవులОценок пока нет
- JBB2012 949048Документ11 страницJBB2012 949048సాయిమహేష్రెడ్డిఆవులОценок пока нет
- JBB2012 949048Документ11 страницJBB2012 949048సాయిమహేష్రెడ్డిఆవులОценок пока нет
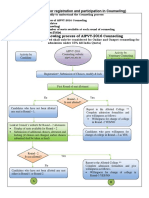
- Counseling Procedure On WebДокумент2 страницыCounseling Procedure On Webసాయిమహేష్రెడ్డిఆవులОценок пока нет
- Seat Matrix 2016Документ4 страницыSeat Matrix 2016సాయిమహేష్రెడ్డిఆవులОценок пока нет
- Houston-2011-The Journal of Clinical HypertensionДокумент7 страницHouston-2011-The Journal of Clinical Hypertensionసాయిమహేష్రెడ్డిఆవులОценок пока нет
- WBJEE Biology SolutionДокумент9 страницWBJEE Biology SolutionsanjaywasanОценок пока нет
- User'S Manual FOR Candidates FOR: Online Registration & Choice FillingДокумент16 страницUser'S Manual FOR Candidates FOR: Online Registration & Choice Fillingసాయిమహేష్రెడ్డిఆవులОценок пока нет
- College Details As On 2016Документ10 страницCollege Details As On 2016సాయిమహేష్రెడ్డిఆవులОценок пока нет
- Frequently Asked Questions (Faqs)Документ7 страницFrequently Asked Questions (Faqs)సాయిమహేష్రెడ్డిఆవులОценок пока нет
- Technote 7 Teat DisinfectionДокумент20 страницTechnote 7 Teat Disinfectionసాయిమహేష్రెడ్డిఆవుల100% (1)
- Bitumen With Salt PDFДокумент9 страницBitumen With Salt PDFbkswain2003Оценок пока нет
- Learning Targets and Success CriteriaДокумент10 страницLearning Targets and Success Criteriaapi-310199974Оценок пока нет
- MSC Thesis - M.SartawiДокумент68 страницMSC Thesis - M.Sartawiااا لالاОценок пока нет
- Formation of BenzeneДокумент39 страницFormation of BenzenehfrizviОценок пока нет
- Waiver For RespondentsДокумент5 страницWaiver For RespondentsJayb See TacadenaОценок пока нет
- Resins and IntermediatesДокумент6 страницResins and IntermediatesDhruv SevakОценок пока нет
- Unleashing Your Potential With Unique SAT PrepДокумент18 страницUnleashing Your Potential With Unique SAT Preppreeti.testprepkartОценок пока нет
- Apga Code of Environmental Practice PDFДокумент130 страницApga Code of Environmental Practice PDFmichaelsullivan1973Оценок пока нет
- If You Find Any Errors, Please Let Your Instructor Know ASAPДокумент3 страницыIf You Find Any Errors, Please Let Your Instructor Know ASAPParesh Kumar SahooОценок пока нет
- Machines That Kill - Saberhagen, Fred, 1930-2007 Greenberg, Martin Harry - New York, 1984 - New York - Ace Science Fiction Books - 9780441513581 - Anna's ArchiveДокумент340 страницMachines That Kill - Saberhagen, Fred, 1930-2007 Greenberg, Martin Harry - New York, 1984 - New York - Ace Science Fiction Books - 9780441513581 - Anna's ArchiveTron TronОценок пока нет
- Energetics Explained: Exothermic vs Endothermic ReactionsДокумент12 страницEnergetics Explained: Exothermic vs Endothermic ReactionsAliyah HamiltonОценок пока нет
- The Use of 1% Nano-Fe3O4 and 1% Nano-TiO2 As Partial Replacement of Cement To Enhance The Chemical Performance of Reinforced Concrete StructuresДокумент12 страницThe Use of 1% Nano-Fe3O4 and 1% Nano-TiO2 As Partial Replacement of Cement To Enhance The Chemical Performance of Reinforced Concrete StructuresCamila Marçal GobiОценок пока нет
- IEM Mid Semester Exam QuestionsДокумент3 страницыIEM Mid Semester Exam QuestionsK38Aryya BhattacharyaCSBSОценок пока нет
- Learning Guide Unit 8: Discussion AssignmentДокумент4 страницыLearning Guide Unit 8: Discussion AssignmentChrispine Mukuka MwambaОценок пока нет
- EHS DOC 001 - LaboratorySafetyManualДокумент94 страницыEHS DOC 001 - LaboratorySafetyManualankur_haldarОценок пока нет
- Crime Scene Decoders Algebra: Polynomials: Standard Focus: Time Range: Supplies: Topics of FocusДокумент14 страницCrime Scene Decoders Algebra: Polynomials: Standard Focus: Time Range: Supplies: Topics of Focusdrecosh-1Оценок пока нет
- Topic Introduction To Chipko Silent Valley Movement and BishnoisДокумент15 страницTopic Introduction To Chipko Silent Valley Movement and BishnoisHarshal BharatiОценок пока нет
- Dry Air Gas PropertiesДокумент25 страницDry Air Gas Propertiesmshah222Оценок пока нет
- Essential Oil of Ginger (Zingiber Officinale Roscoe) - Libgen - LiДокумент22 страницыEssential Oil of Ginger (Zingiber Officinale Roscoe) - Libgen - Liaghiasophie100% (1)
- 4 - Linguistic AnalogyДокумент20 страниц4 - Linguistic AnalogyAniala DequinaОценок пока нет
- UntitledДокумент49 страницUntitledKhanh Trương Lê MaiОценок пока нет
- Bonaventure ResumeДокумент1 страницаBonaventure Resumeapi-631877498Оценок пока нет
- The Life of Pleaure - ScriptДокумент2 страницыThe Life of Pleaure - ScriptQueen Anne Mhajheelah MagcuroОценок пока нет
- University of Groningen MagazineДокумент17 страницUniversity of Groningen Magazine林忠緯Оценок пока нет
- Textbooks: 1. Pallab Bhattacharya "Semiconductor Opto Electronic Devices", Prentice Hall of India PVT.Документ1 страницаTextbooks: 1. Pallab Bhattacharya "Semiconductor Opto Electronic Devices", Prentice Hall of India PVT.Petrishia ArockiasamyОценок пока нет
- SECTION 21 - MicropilingДокумент8 страницSECTION 21 - MicropilingTony JamesОценок пока нет